Department of Thoracic Surgery, Kansai Medical University, Hirakata, Osaka, Japan.
Nursing Department, Kansai Medical University Hospital, Hirakata, Osaka, Japan.
PLoS One. 2023 Feb 22;18(2):e0281998. doi: 10.1371/journal.pone.0281998. eCollection 2023.
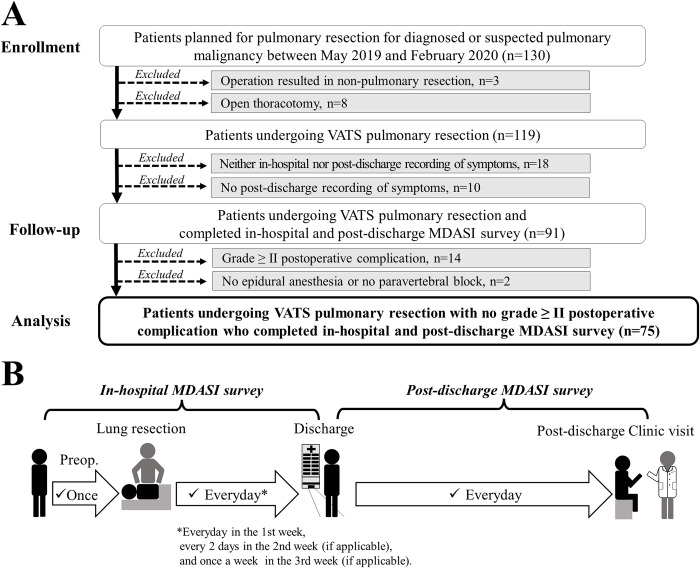
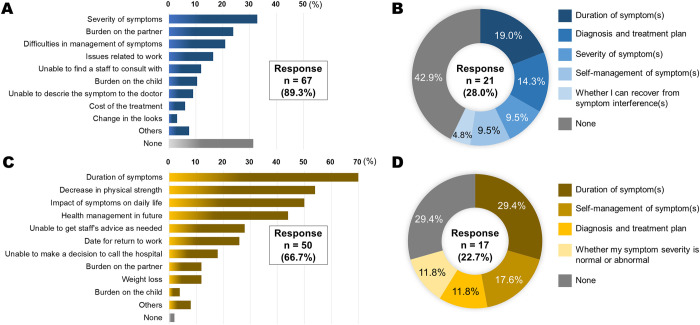
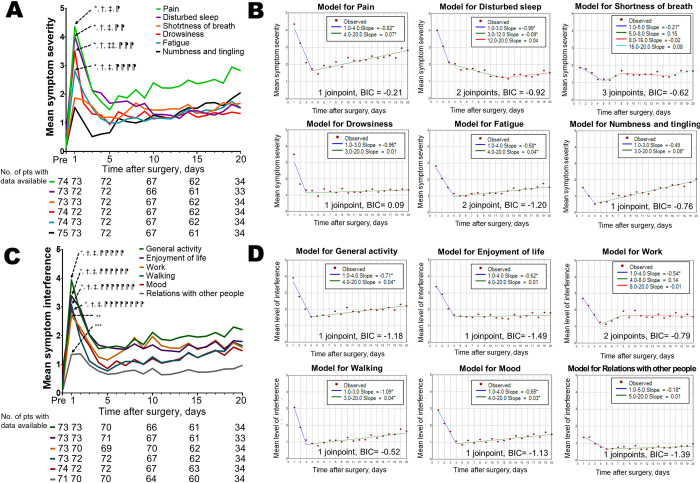
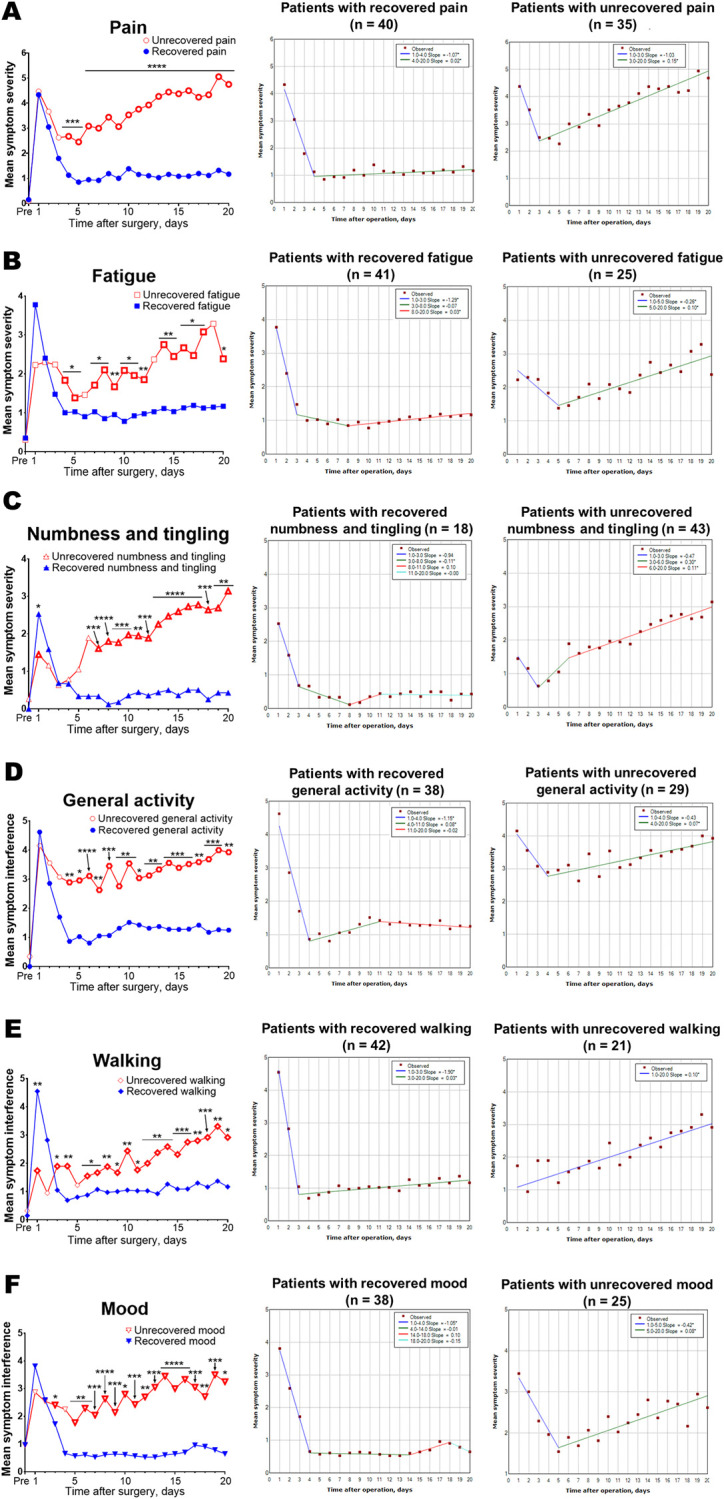
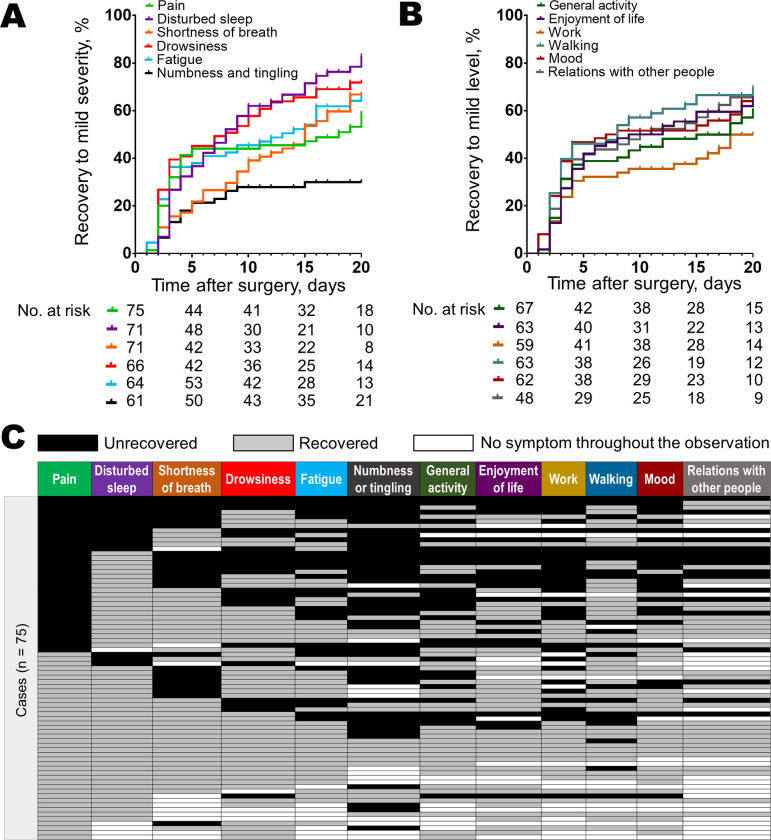
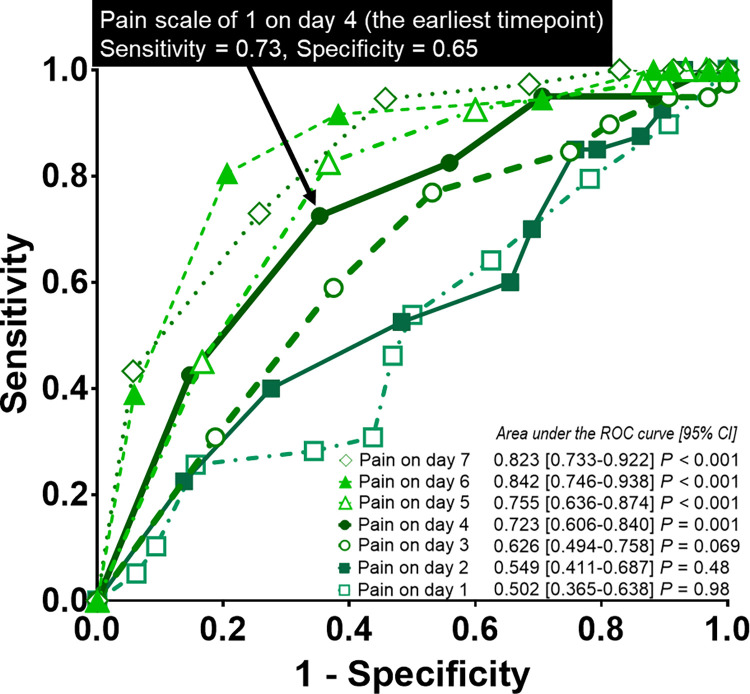
This study aimed to characterize patients' symptom severity trajectories and distresses from video-assisted thoracoscopic lung resection to the first post-discharge clinic visit. Seventy-five patients undergoing thoracoscopic lung resection for diagnosed or suspected pulmonary malignancy prospectively recorded daily symptom severity on a 0-10 numeric scale using the MD Anderson Symptom Inventory until the first post-discharge clinic visit. The causes of postoperative distresses were surveyed, and symptom severity trajectories were analyzed using joinpoint regression. A rebound was defined as a statistically significant positive slope after a statistically significant negative slope. Symptom recovery was defined as symptom severity of ≤3 in two contiguous measurements. The accuracy of pain severity on days 1-5 for predicting pain recovery was determined using area under the receiver operating characteristic curves. We applied Cox proportional hazards models for multivariate analyses of the potential predictors of early pain recovery. The median age was 70 years, and females accounted for 48%. The median interval from surgery to the first post-discharge clinic visit was 20 days. Trajectories of several core symptoms including pain showed a rebound from day 3 or 4. Specifically, pain severity in patients with unrecovered pain had been higher than those with recovered pain since day 4. Pain severity on day 4 showed the highest area under the curve of 0.723 for predicting pain recovery (P = 0.001). Multivariate analysis identified pain severity of ≤1 on day 4 as an independent predictor of early pain recovery (hazard ratio, 2.86; P = 0.0027). Duration of symptom was the leading cause of postoperative distress. Several core symptoms after thoracoscopic lung resection showed a rebound in the trajectory. Specifically, a rebound in pain trajectory may be associated with unrecovered pain; pain severity on day 4 may predict early pain recovery. Further clarification of symptom severity trajectories is essential for patient-centered care.
本研究旨在描述患者从电视辅助胸腔镜肺切除术后到首次出院后就诊期间的症状严重程度轨迹和困扰。75 例接受电视辅助胸腔镜肺切除术治疗诊断或疑似肺部恶性肿瘤的患者前瞻性地使用 MD 安德森症状量表以 0-10 的数字量表记录每日症状严重程度,直到首次出院后就诊。调查了术后困扰的原因,并使用 joinpoint 回归分析了症状严重程度轨迹。反弹定义为在统计学上显著的负斜率之后出现统计学上显著的正斜率。症状恢复定义为连续两次测量的症状严重程度≤3。使用接收者操作特征曲线下的面积确定疼痛严重程度在第 1-5 天对预测疼痛恢复的准确性。我们应用 Cox 比例风险模型对早期疼痛恢复的潜在预测因素进行多变量分析。中位年龄为 70 岁,女性占 48%。手术到首次出院后就诊的中位间隔为 20 天。包括疼痛在内的几种核心症状的轨迹均显示从第 3 天或第 4 天开始反弹。具体而言,未恢复疼痛患者的疼痛严重程度自第 4 天以来一直高于已恢复疼痛的患者。第 4 天的疼痛严重程度预测疼痛恢复的曲线下面积最高,为 0.723(P = 0.001)。多变量分析确定第 4 天的疼痛严重程度≤1 是早期疼痛恢复的独立预测因素(危险比,2.86;P = 0.0027)。症状持续时间是术后困扰的主要原因。胸腔镜肺切除术后的几种核心症状在轨迹上出现反弹。具体而言,疼痛轨迹的反弹可能与未恢复的疼痛有关;第 4 天的疼痛严重程度可能预测早期疼痛恢复。进一步阐明症状严重程度轨迹对于以患者为中心的护理至关重要。