Nie Shanmao, Fu Shangyu, Fang Kaiyan
Department of Hepatobiliary Surgery, Luzhou people's Hospital, Luzhou, China.
Department of Anesthesiology, Luzhou people's Hospital, Luzhou, China.
Front Surg. 2023 Feb 3;10:1124955. doi: 10.3389/fsurg.2023.1124955. eCollection 2023.
Cholelithiasis is a frequently occurring disease in clinic. Due to changes in people's living environments, dietary habits and the aging population, cholelithiasis incidence is increasing. Currently, laparoscopic cholecystectomy (LC) is the preferred treatment for gallbladder stones, but the surgical method for patients with choledocholithiasis is controversial. An endoscopic retrograde cholangiopancreatography (pERCP) is performed preoperatively, followed by LC as the general treatment method. However, pERCP still has some disadvantages, such as prolonged hospital stay, increased incidence of postoperative pancreatitis, and increased duration of anesthesia. Therefore, intraoperative endoscopic retrograde cholangiopancreatography (iERCP) is proposed.
To compare the efficacy and safety of one-stage treatment and two-stage treatment for the management of patients with cholecystolithiasis and choledocholithiasis.
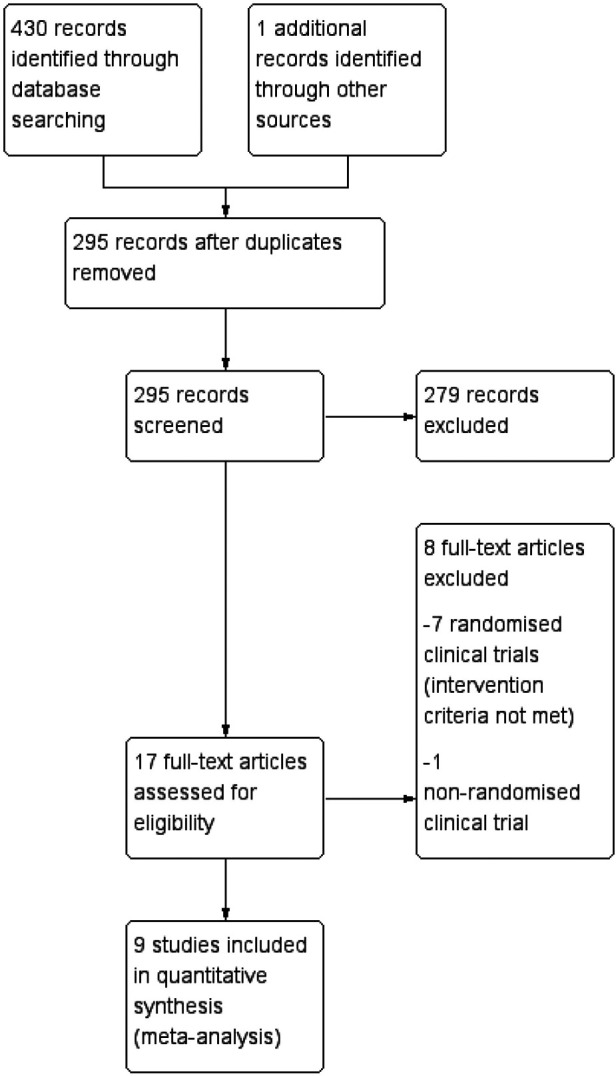
PubMed, Embase, Web of Science, and Cochrane databases were searched through October 2022. The search terms include cholangiolithiasis/bile duct stones/calculi, endoscopic retrograde cholangiopancreatography/ERCP, endoscopic sphincterotomy/EST, laparoendoscopic rendezvous (LERV), and laparoscopic cholecystectomy/LC.
For the treatment of patients with cholecystolithiasis and choledocholithiasis in adults, randomized controlled trials (RCTs) comparing LC with iERCP vs. pERCP followed by LC were conducted.
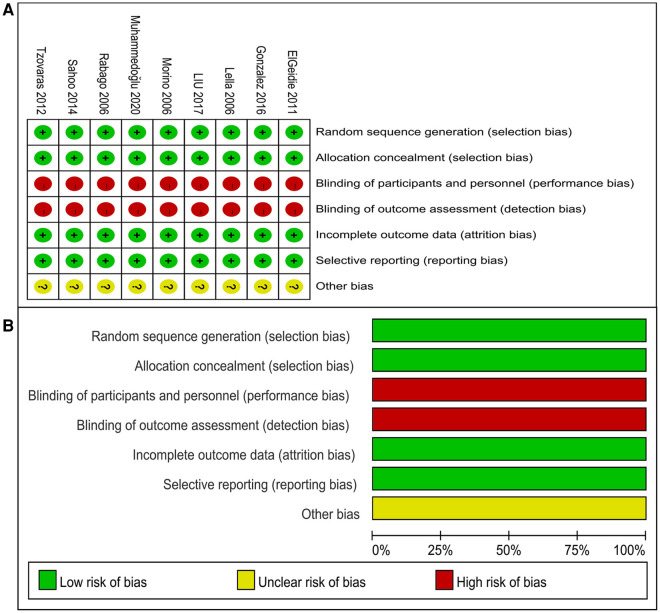
Data extraction and quality assessment were performed by two reviewers. We used Revman version 5.3 to analyze the collected data. The trials were grouped according to the evaluation results such as the overall mortality rate, overall morbidity rate, clearance rate of choledocholithiasis, incidence of pancreatitis, the length of hospitalization, and the length of operation.
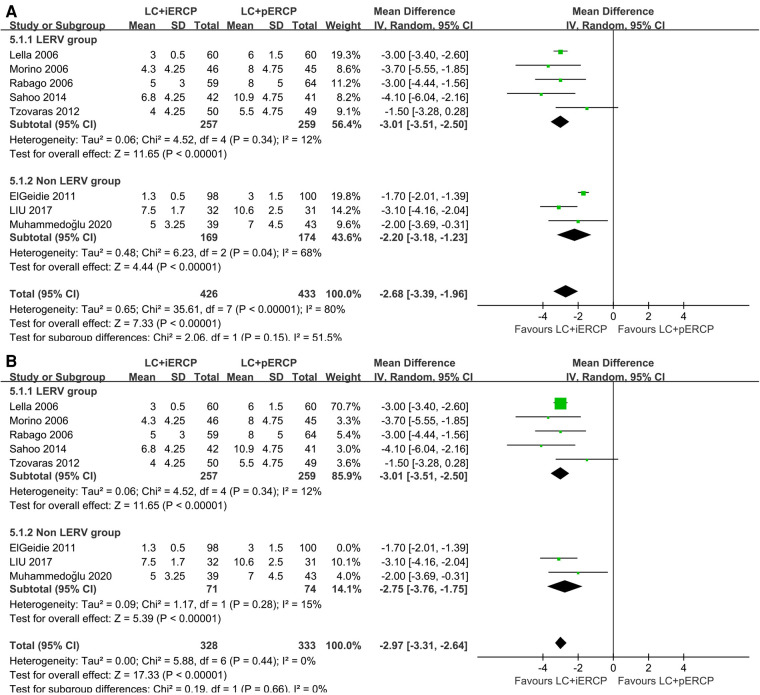
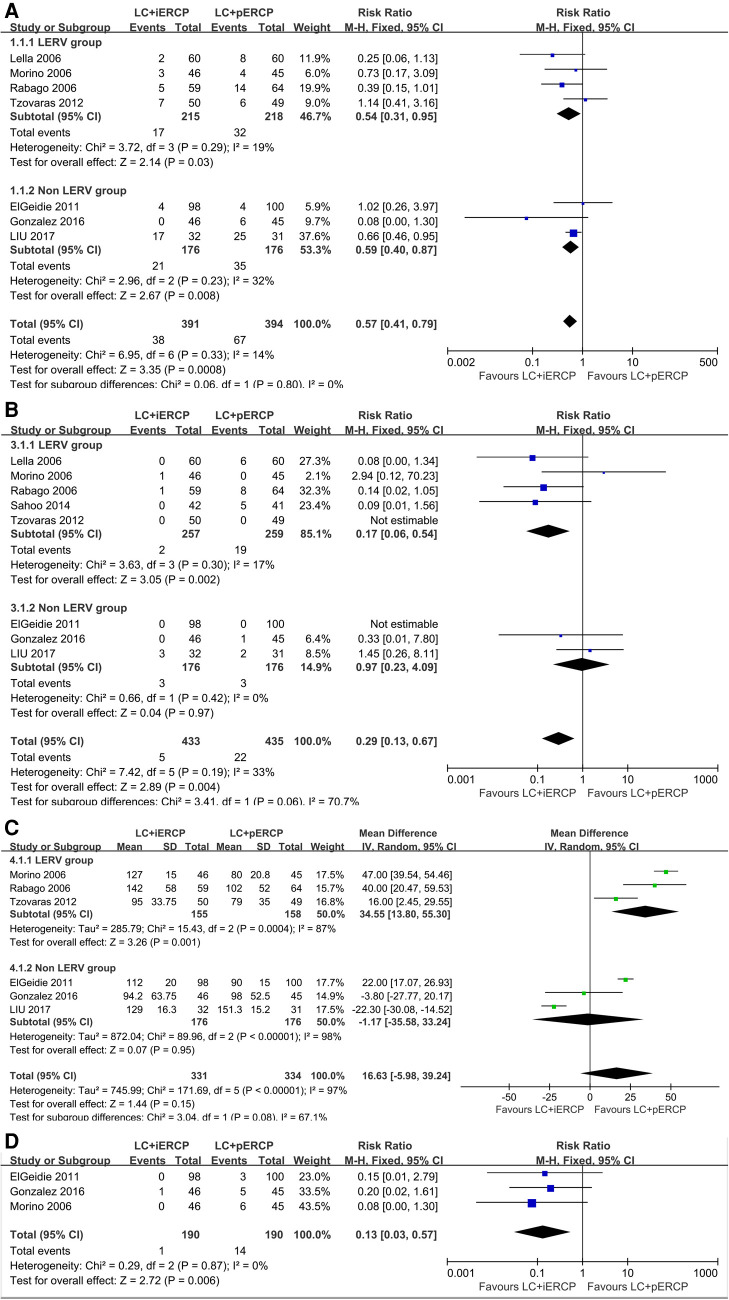
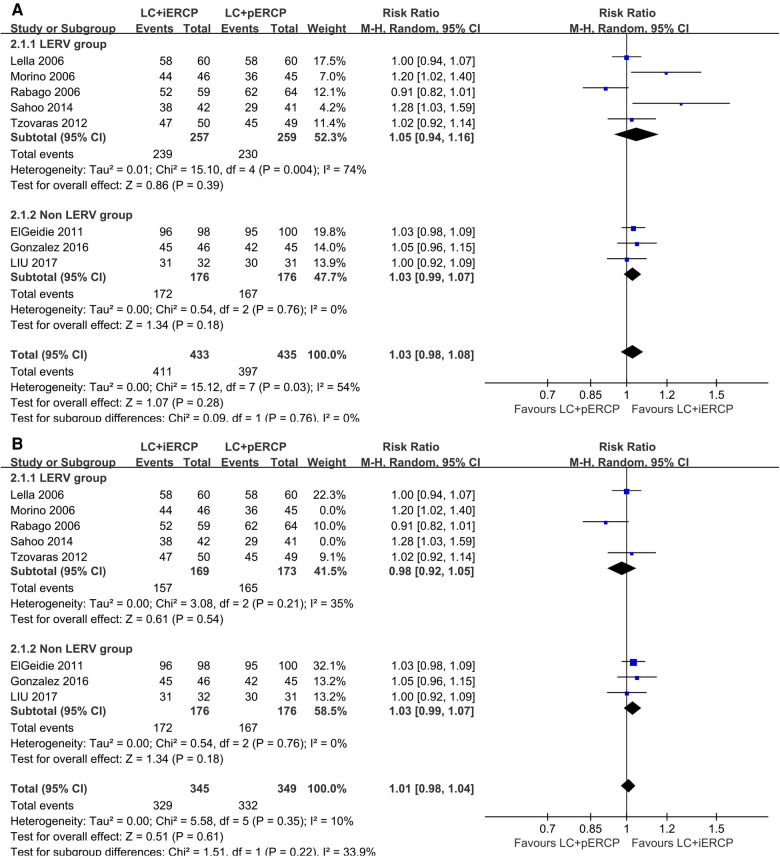
9 RCTs (950 participants) were included in this meta-analyses. The overall morbidity rate in LC + iERCP group is lower than that in LC + pERCP group (RR: 0.57, 95% CI = 0.41-0.79, = 0.0008). The clearance rate of choledocholithiasis in LC + iERCP group was almost the same as that in LC + pERCP group (RR: 1.03, 95% CI = 0.98-1.08, = 0.28). The incidence of pancreatitis in LC + iERCP group is lower than that in LC + pERCP group (RR: 0.29, 95% CI = 0.13-0.67, = 0.004). The length of operation of the LC + iERCP group seems to be similar to that of the LC + pERCP group (MD: 16.63 95% CI = -5.98-39.24, = 0.15). LC + iERCP group has a shorter length of hospitalization than that in LC + pERCP group (MD: -2.68 95% CI = -3.39--1.96, < 0.00001). LC + iERCP group has lower postoperative second ERCP rate than that in LC + pERCP group (RR: 0.13, 95% CI = 0.03-0.57, = 0.006).
Our study suggest that LC + iERCP may be a better option than LC + pERCP in the management of patients with both cholecystolithiasis and choledocholithiasis. This procedure can reduce the overall incidence of postoperative complications, especially the occurrence of postoperative pancreatitis. It could shorten the length of hospital stay, reduce postoperative second ERCP rate.
胆石症是临床上的一种常见疾病。由于人们生活环境、饮食习惯的改变以及人口老龄化,胆石症的发病率正在上升。目前,腹腔镜胆囊切除术(LC)是胆囊结石的首选治疗方法,但胆总管结石患者的手术方式存在争议。通常的治疗方法是术前进行内镜逆行胰胆管造影(pERCP),然后进行LC。然而,pERCP仍存在一些缺点,如住院时间延长、术后胰腺炎发病率增加以及麻醉时间延长。因此,有人提出术中内镜逆行胰胆管造影(iERCP)。
比较一期治疗和二期治疗胆囊结石合并胆总管结石患者的疗效和安全性。
检索了截至2022年10月的PubMed、Embase、Web of Science和Cochrane数据库。检索词包括胆管结石/胆总管结石/结石、内镜逆行胰胆管造影/ERCP、内镜括约肌切开术/EST、腹腔镜内镜会师术(LERV)以及腹腔镜胆囊切除术/LC。
针对成人胆囊结石合并胆总管结石患者的治疗,进行了比较LC与iERCP对比pERCP联合LC的随机对照试验(RCT)。
由两名评价者进行数据提取和质量评估。我们使用Revman 5.3版分析收集到的数据。根据总死亡率、总发病率、胆总管结石清除率、胰腺炎发病率、住院时间和手术时间等评估结果对试验进行分组。
本荟萃分析纳入了9项RCT(950名参与者)。LC+iERCP组的总发病率低于LC+pERCP组(RR:0.57,95%CI=0.41-0.79,P=0.0008)。LC+iERCP组的胆总管结石清除率与LC+pERCP组几乎相同(RR:1.03,95%CI=0.98-1.08,P=0.28)。LC+iERCP组的胰腺炎发病率低于LC+pERCP组(RR:0.29,95%CI=0.13-0.67,P=0.004)。LC+iERCP组的手术时间似乎与LC+pERCP组相似(MD:16.63,95%CI=-5.98-39.24,P=0.15)。LC+iERCP组的住院时间比LC+pERCP组短(MD:-2.68,95%CI=-3.39--1.96,P<0.00001)。LC+iERCP组的术后二次ERCP率低于LC+pERCP组(RR:0.13,95%CI=0.03-0.57,P=0.006)。
我们的研究表明,在治疗胆囊结石合并胆总管结石患者时,LC+iERCP可能是比LC+pERCP更好的选择。该手术可降低术后并发症的总体发生率,尤其是术后胰腺炎的发生。它可以缩短住院时间,降低术后二次ERCP率。