Max Delbruck Centre for Molecular Medicine, Berlin, Germany.
Max Delbruck Centre for Molecular Medicine, Berlin, Germany
J Immunother Cancer. 2023 Feb;11(2). doi: 10.1136/jitc-2022-006001.
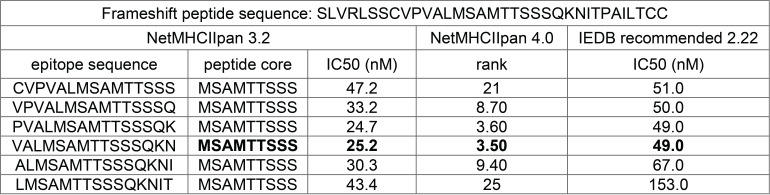
Adoptive transfer of patient's T cells, engineered to express a T cell receptor (TCR) with defined novel antigen specificity, is a convenient form of cancer therapy. In most cases, major histocompatibility complex (MHC) I-restricted TCRs are expressed in CD8 T cells and the development of CD4 T cells engineered to express an MHC II-restricted TCR lacks behind. Critical is the choice of the target antigen, whether the epitope is efficiently processed and binds with high affinity to MHC molecules. A mutation in the transforming growth factor β receptor 2 (TGFβR2(-1)) gene creates a frameshift peptide caused by the deletion of one adenine (-1) within a microsatellite sequence. This somatic mutation is recurrent in microsatellite instable colorectal and gastric cancers and, therefore, is a truly tumor-specific antigen detected in many patients.
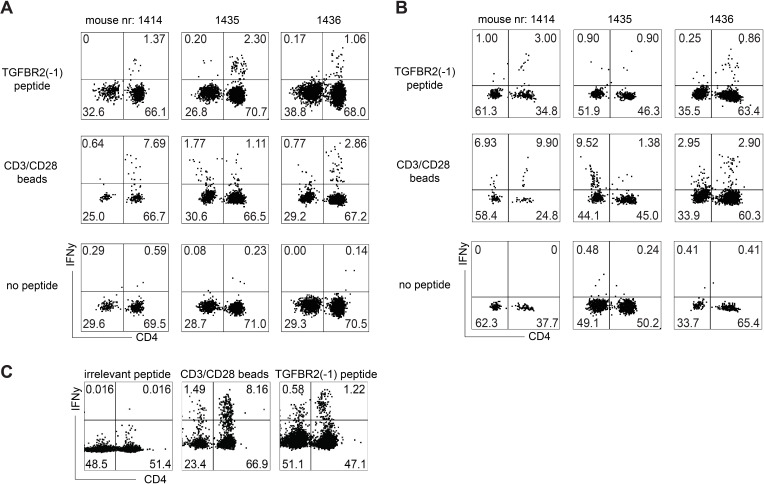
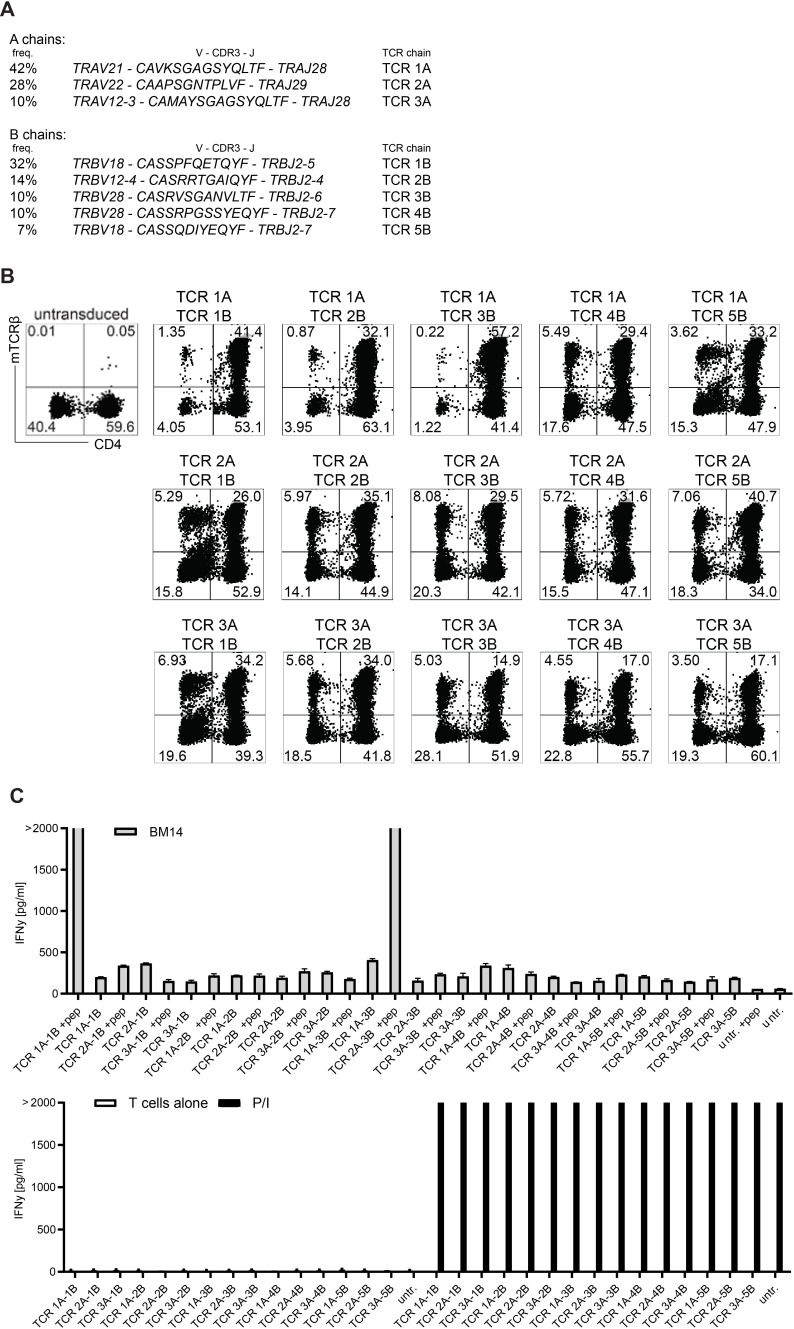
ABabDR4 mice, which express a diverse human TCR repertoire restricted to human MHC II molecule HLA-DRA/DRB1*0401 (HLA-DR4), were immunized with the TGFβR2(-1) peptide and TGFβR2(-1)-specific TCRs were isolated from responding CD4 T cells. The TGFβR2(-1)-specific TCRs were expressed in human CD4 T cells and their potency and safety profile were assessed by co-cultures and other functional assays.
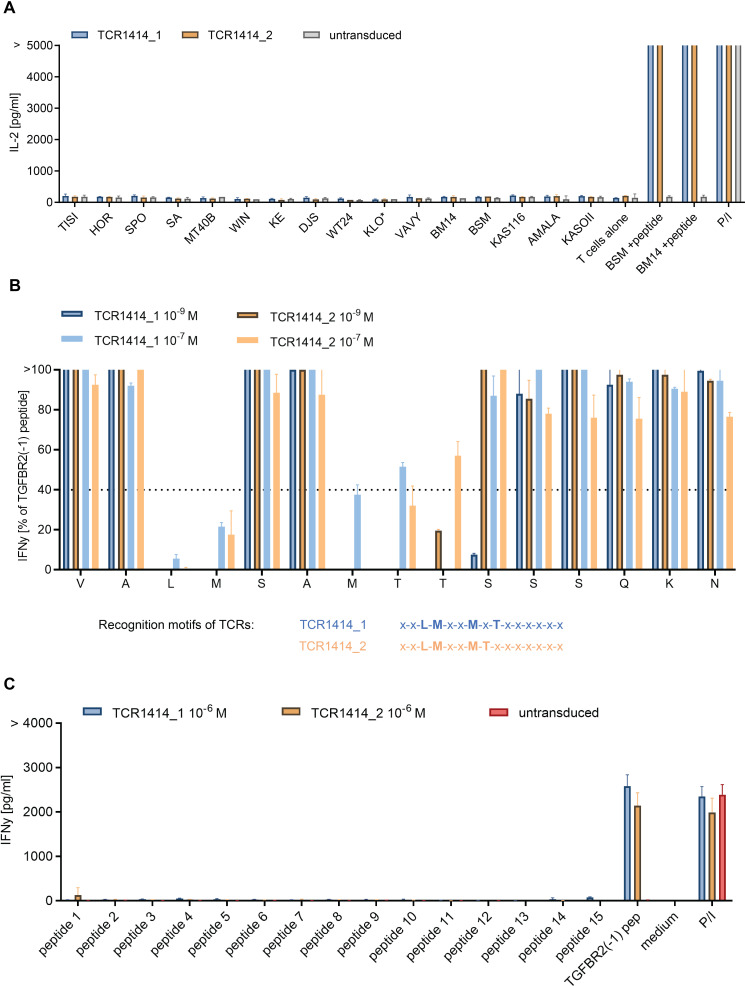
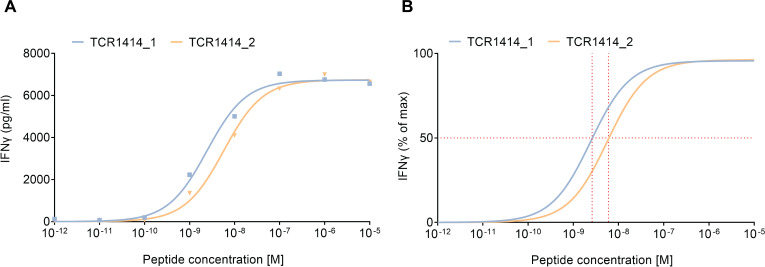
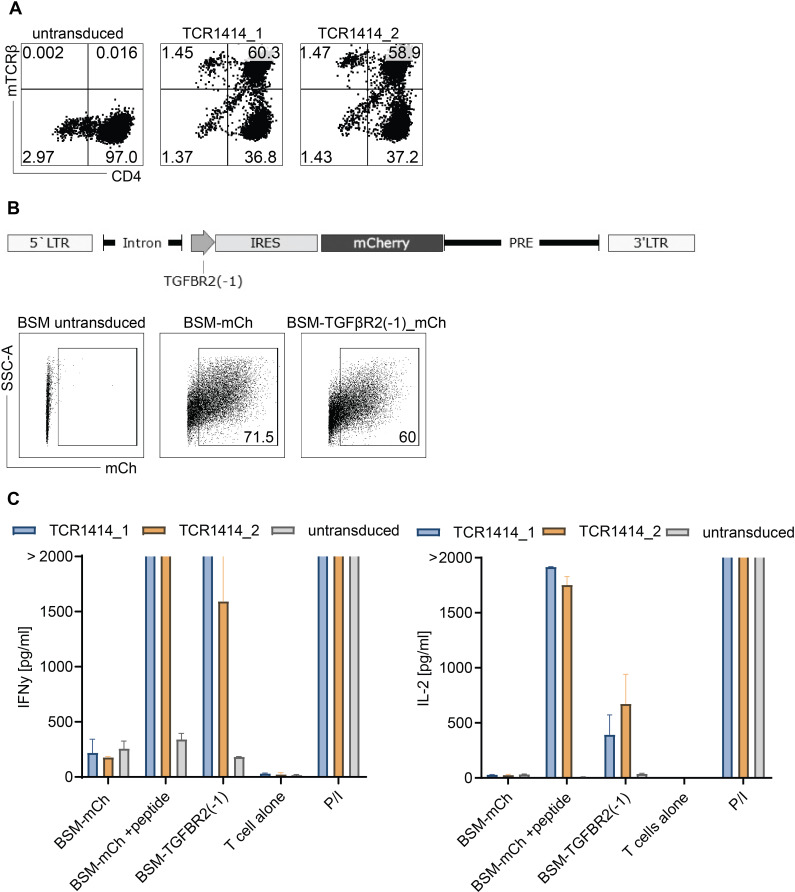
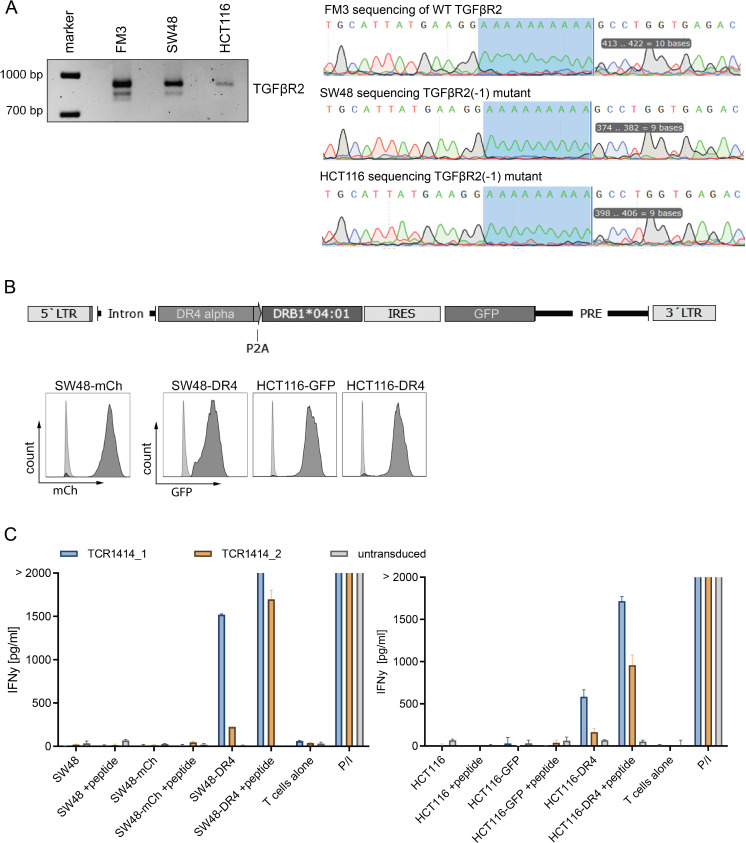
We demonstrated that TGFβR2(-1) neoantigen is immunogenic and elicited CD4 T cell responses in ABabDR4 mice. When expressed in human CD4 T cells, the HLA-DR4 restricted TGFβR2(-1)-specific TCRs induced IFNy expression at low TGFβR2(-1) peptide amounts. The TGFβR2(-1)-specific TCRs recognized HLA-DR4 lymphoblastoid cells, which endogenously processed and presented the neoantigen, and colorectal cancer cell lines SW48 and HCT116 naturally expressing the TGFβR2(-1) mutation. No MHC II alloreactivity or cross-reactivity to peptides with a similar TCR-recognition motif were observed, indicating the safety of the TCRs.
The data suggest that HLA-DR4-restricted TCRs specific for the TGFβR2(-1) recurrent neoantigen can be valuable candidates for adoptive T cell therapy of a sizeable number of patients with cancer.
过继转移经基因工程修饰表达具有特定抗原新特异性的 T 细胞受体(TCR)的方法是一种方便的癌症治疗形式。在大多数情况下,主要组织相容性复合体(MHC)I 限制性 TCR 表达在 CD8 T 细胞中,而表达 MHC II 限制性 TCR 的 CD4 T 细胞的工程化发展则落后。关键是选择靶抗原,抗原表位是否能被有效加工,以及是否能与 MHC 分子以高亲和力结合。转化生长因子 β 受体 2(TGFβR2(-1)) 基因的突变会导致一个微卫星序列中一个腺嘌呤(-1)的缺失,从而产生一个移码肽。这种体细胞突变在微卫星不稳定的结直肠癌和胃癌中反复出现,因此是一种在许多患者中检测到的真正肿瘤特异性抗原。
ABabDR4 小鼠表达一种多样化的人类 TCR repertoire,受限于人类 MHC II 分子 HLA-DRA/DRB1*0401(HLA-DR4),用 TGFβR2(-1) 肽免疫,从反应性 CD4 T 细胞中分离出 TGFβR2(-1)- 特异性 TCR。将 TGFβR2(-1)- 特异性 TCR 表达在人类 CD4 T 细胞中,并通过共培养和其他功能测定评估其效力和安全性。
我们证明 TGFβR2(-1) 新抗原是免疫原性的,并在 ABabDR4 小鼠中引起 CD4 T 细胞反应。当在人类 CD4 T 细胞中表达时,HLA-DR4 限制性 TGFβR2(-1)- 特异性 TCR 在低 TGFβR2(-1) 肽量下诱导 IFNy 表达。TGFβR2(-1)- 特异性 TCR 识别内源性加工和呈递新抗原的 HLA-DR4 淋巴母细胞系,以及天然表达 TGFβR2(-1) 突变的结直肠癌细胞系 SW48 和 HCT116。未观察到 MHC II 同种异体反应或对具有类似 TCR 识别基序的肽的交叉反应性,表明 TCR 的安全性。
数据表明,针对 TGFβR2(-1) 反复出现的新抗原的 HLA-DR4 限制性 TCR 可能是为数众多的癌症患者过继性 T 细胞治疗的有价值的候选物。