Women's Health and Perinatology Research Group, Department of Clinical Medicine, Faculty of Health Sciences, UiT-The Arctic University of Norway, Tromsø, Norway.
Department of Obstetrics and Gynecology, University Hospital of North Norway, Tromsø, Norway.
Acta Obstet Gynecol Scand. 2023 Mar;102(3):270-281. doi: 10.1111/aogs.14525.
The burden of perinatal mental health problems was expected to increase during the COVID-19 pandemic. We prospectively investigated the impact of the COVID-19 pandemic on the mental health of pregnant and postpartum women in Norway and explored associations with their sociodemographic characteristics and personality traits.
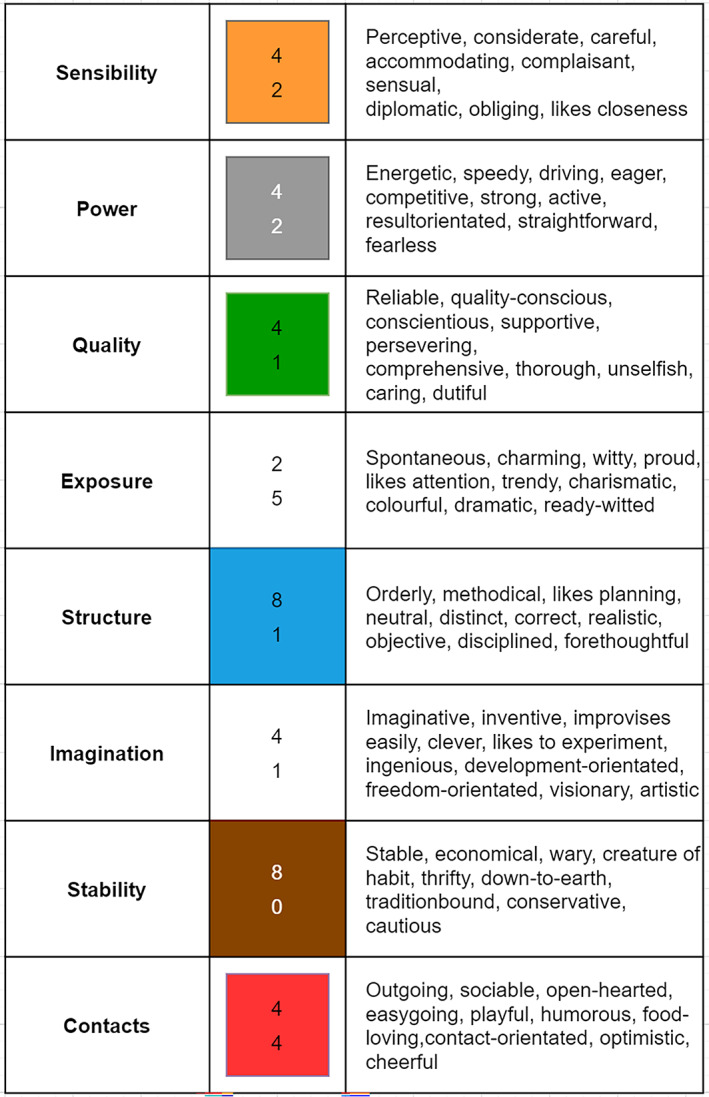
Sociodemographic information and the self-reported impact of pandemic on wellbeing of pregnant women was collected using an online survey. To assess women's mental health, two validated questionnaires, the Edinburgh Postpartum Depression Scale (EPDS) and the Generalized Anxiety Disorder-7 item Scale (GAD-7), were used prenatally and postnatally. Personality traits were evaluated using HumanGuide, a web-based ipsative psychological evaluation instrument.
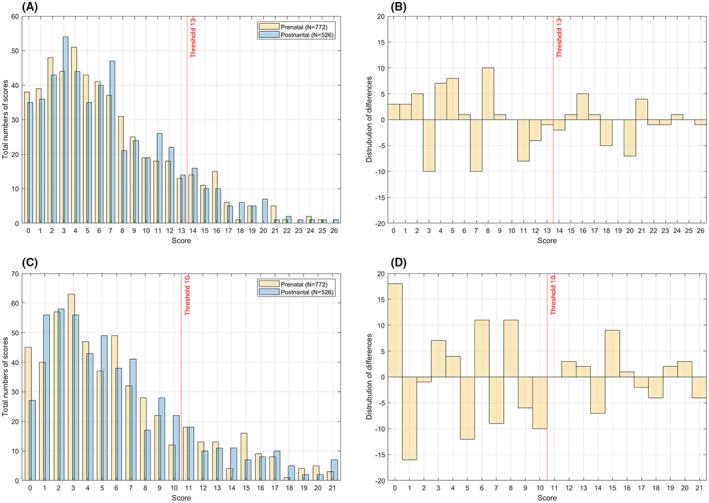
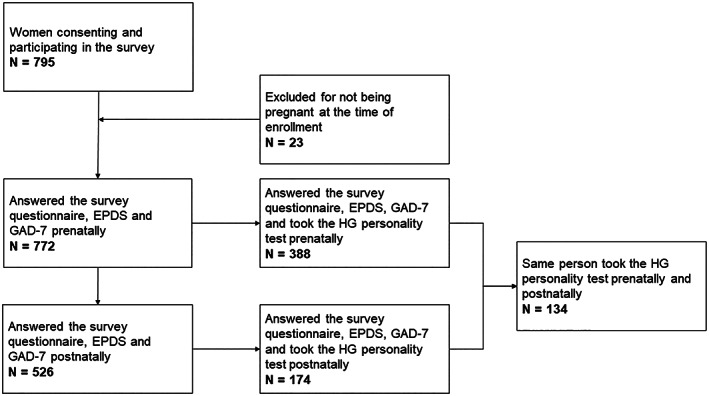
772 women were included prenatally, of which 526 also responded to the survey 4-6 weeks postnatally. The median age was 29 years, 53.6% of the women were nulliparous when enrolled, and 35.1% worked in the healthcare sector. The median EPDS (6.0; interquartile range [IQR] 3.0-10.0 vs 6.0; IQR: 3.0-10.0) and the median GAD-7 (5.0; IQR 2.0-9.0 vs 5.0; IQR 2.0-9.0) were similar pre-and postnatally. Prenatally, the proportion of women scoring ≥13 on EPDS and ≥10 on GAD-7 was 14.5% (112/772) and 21.5% (166/772), whereas the postnatal figures were 15.6% (82/526) and 21.5% (113/526), respectively. The differences were not significant (P = 0.59 and P = 0.99). Being <25 years of age, being on pre-pregnancy psychotherapy or psychotropic medication, frequent voluntary isolation, perception of maternity care not proceeding normally, avoiding seeking medical assistance due to fear of infection and having negative economic consequences during the COVID19 pandemic significantly increased the risk of both anxiety (GAD-7 ≥10) and depression (EPDS ≥13). Nullipara had a higher risk of anxiety, whereas being a healthcare worker had a lower risk. The personality trait factors Power (P = 0.008), Quality (P = 0.008), Stability (P < 0.001) and Contacts (P < 0.001) were significant predictors of depression among pregnant women, whereas the Quality (P = 0.005) and Contacts (P = 0.003) were significant predictors of anxiety.
During the initial phase of the COVID-19 pandemic, the prevalence of depression (EPDS ≥ 13) and anxiety (GAD-7 ≥ 10) was 14.5% and 21.5%, respectively, among Norwegian pregnant women. Certain sociodemographic characteristics and personality traits were significant predictors of depression and anxiety.
在 COVID-19 大流行期间,围产期心理健康问题的负担预计会增加。我们前瞻性地调查了 COVID-19 大流行对挪威孕妇和产后妇女心理健康的影响,并探讨了其与社会人口特征和人格特质的关联。
使用在线调查收集孕妇的社会人口信息和大流行对幸福感的影响。为了评估女性的心理健康,我们使用了两个经过验证的问卷,爱丁堡产后抑郁量表(EPDS)和广泛性焦虑障碍-7 项量表(GAD-7),分别在产前和产后进行评估。人格特质使用 HumanGuide 进行评估,HumanGuide 是一种基于网络的特质心理评估工具。
772 名女性在产前被纳入研究,其中 526 名女性在产后 4-6 周也回复了调查。中位年龄为 29 岁,53.6%的女性在入组时为初产妇,35.1%的女性在医疗保健部门工作。产前 EPDS(6.0;四分位距 [IQR] 3.0-10.0 vs 6.0;IQR:3.0-10.0)和 GAD-7(5.0;IQR 2.0-9.0 vs 5.0;IQR 2.0-9.0)中位数相似。产前,EPDS 评分≥13 和 GAD-7 评分≥10 的女性比例分别为 14.5%(112/772)和 21.5%(166/772),而产后的比例分别为 15.6%(82/526)和 21.5%(113/526),差异无统计学意义(P=0.59 和 P=0.99)。年龄<25 岁、妊娠前接受心理治疗或精神药物治疗、频繁自愿隔离、感觉孕产护理不正常、因担心感染而避免寻求医疗帮助以及 COVID19 大流行期间出现经济负面影响显著增加了焦虑(GAD-7≥10)和抑郁(EPDS≥13)的风险。初产妇焦虑风险较高,而医护人员焦虑风险较低。人格特质因素权力(P=0.008)、素质(P=0.008)、稳定性(P<0.001)和人脉(P<0.001)是孕妇抑郁的显著预测因素,而素质(P=0.005)和人脉(P=0.003)是焦虑的显著预测因素。
在 COVID-19 大流行的初始阶段,挪威孕妇中抑郁(EPDS≥13)和焦虑(GAD-7≥10)的患病率分别为 14.5%和 21.5%。某些社会人口特征和人格特质是抑郁和焦虑的显著预测因素。