Faculty of Science, School of Life Sciences, University of Technology Sydney, Broadway, NSW 2007, Australia.
Faculty of Medicine, University of Belgrade, 11000 Belgrade, Serbia.
Biomolecules. 2023 Feb 18;13(2):395. doi: 10.3390/biom13020395.
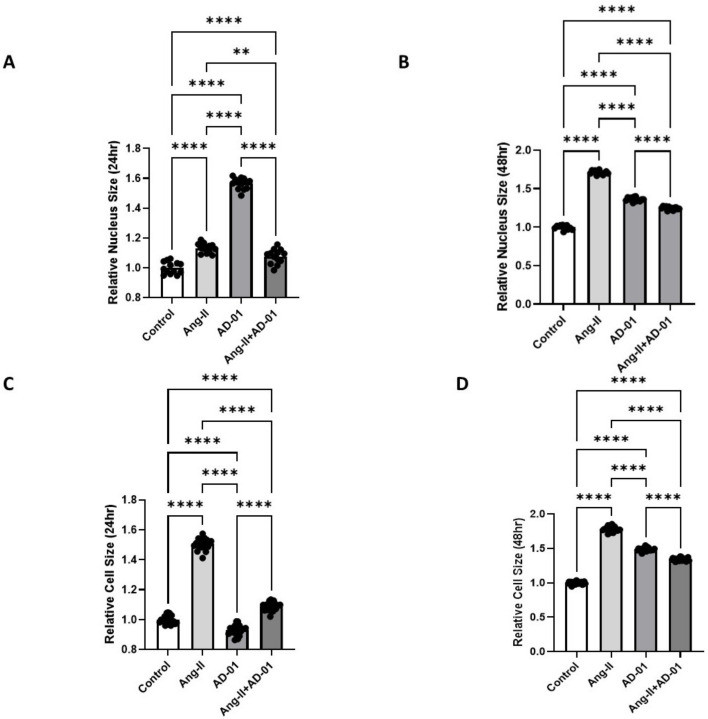
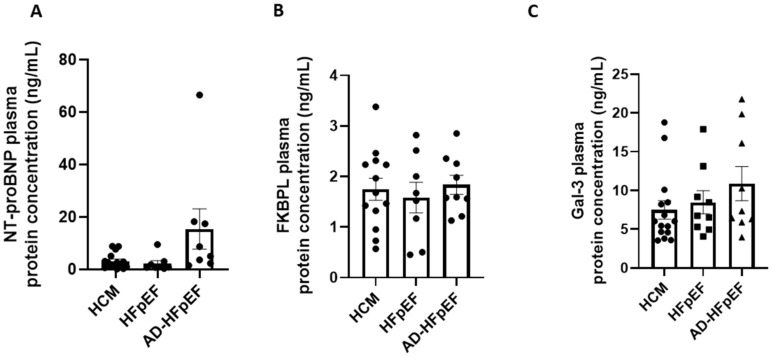
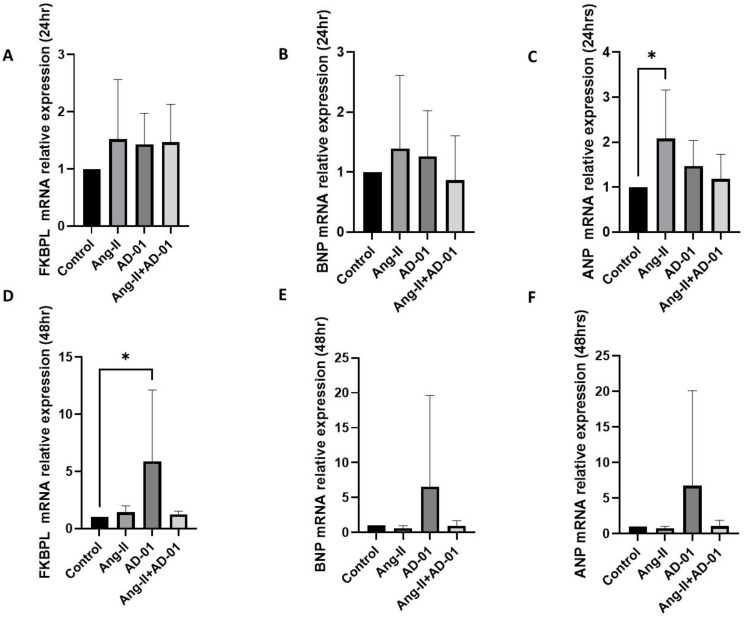
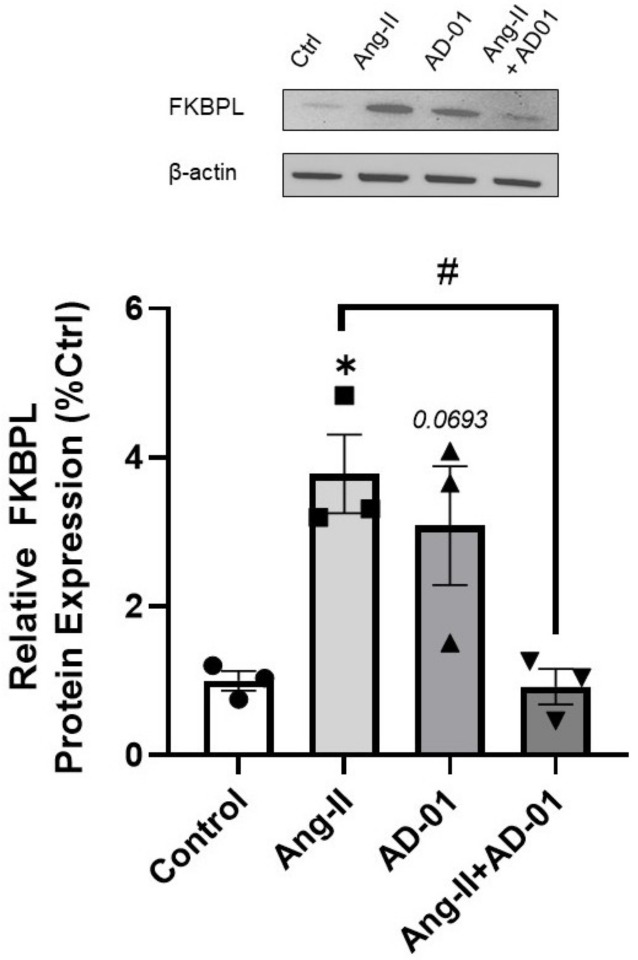
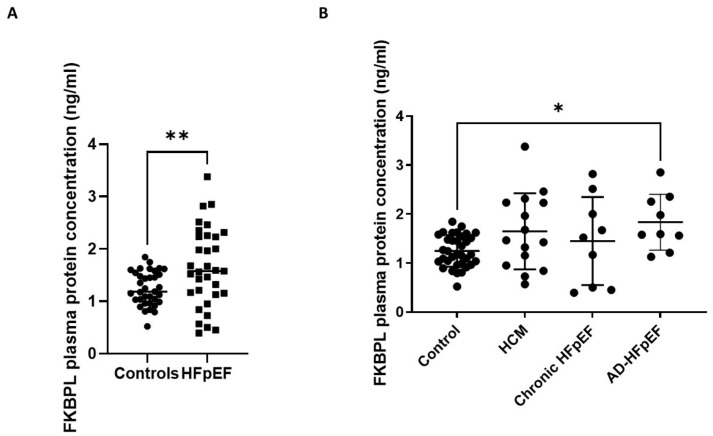
Heart failure (HF) is the leading cause of hospitalisations worldwide, with only 35% of patients surviving the first 5 years after diagnosis. The pathogenesis of HF with preserved ejection fraction (HFpEF) is still unclear, impeding the implementation of effective treatments. FK506-binding protein like (FKBPL) and its therapeutic peptide mimetic, AD-01, are critical mediators of angiogenesis and inflammation. Thus, in this study, we investigated-for the first time-FKBPL's role in the pathogenesis and as a biomarker of HFpEF. In vitro models of cardiac hypertrophy following exposure to a hypertensive stimulus, angiotensin-II (Ang-II, 100 nM), and/or AD-01 (100 nM), for 24 and 48 h were employed as well as human plasma samples from people with different forms of HFpEF and controls. Whilst the FKBPL peptide mimetic, AD-01, induced cardiomyocyte hypertrophy in a similar manner to Ang-II ( < 0.0001), when AD-01 and Ang-II were combined together, this process was abrogated ( < 0.01-0.0001). This mechanism appears to involve a negative feedback loop related to FKBPL ( < 0.05). In human plasma samples, FKBPL concentration was increased in HFpEF compared to controls ( < 0.01); however, similar to NT-proBNP and Gal-3, it was unable to stratify between different forms of HFpEF: acute HFpEF, chronic HFpEF and hypertrophic cardiomyopathy (HCM). FKBPL may be explored for its biomarker and therapeutic target potential in HFpEF.
心力衰竭(HF)是全球住院治疗的主要原因,仅有 35%的患者在诊断后 5 年内存活。射血分数保留的心力衰竭(HFpEF)的发病机制仍不清楚,这阻碍了有效治疗方法的实施。FK506 结合蛋白样(FKBPL)及其治疗性肽类似物 AD-01 是血管生成和炎症的关键介质。因此,在这项研究中,我们首次研究了 FKBPL 在 HFpEF 发病机制中的作用及其作为生物标志物的作用。使用了暴露于高血压刺激物血管紧张素-II(Ang-II,100 nM)和/或 AD-01(100 nM)24 和 48 小时的体外心肌肥厚模型,以及来自不同形式 HFpEF 和对照的人的血浆样本。虽然 FKBPL 肽类似物 AD-01 以类似于 Ang-II 的方式诱导心肌细胞肥大(<0.0001),但当 AD-01 和 Ang-II 一起使用时,这一过程被阻断(<0.01-0.0001)。这种机制似乎涉及与 FKBPL 相关的负反馈环(<0.05)。在人血浆样本中,HFpEF 中的 FKBPL 浓度高于对照组(<0.01);然而,与 NT-proBNP 和 Gal-3 相似,它无法区分不同形式的 HFpEF:急性 HFpEF、慢性 HFpEF 和肥厚型心肌病(HCM)。FKBPL 可作为 HFpEF 的生物标志物和治疗靶点进行探索。