School of Population and Global Health, University of Western Australia, Perth, WA, Australia.
Medical School, University of Western Australia, Perth, WA, Australia.
Eur J Clin Pharmacol. 2023 Apr;79(4):553-567. doi: 10.1007/s00228-023-03467-7. Epub 2023 Feb 28.
Non-adherence to heart failure (HF) medications is associated with poor outcomes. We used restricted cubic splines (RCS) to assess the continuous relationship between adherence to renin-angiotensin system inhibitors (RASI) and β-blockers and long-term outcomes in senior HF patients.
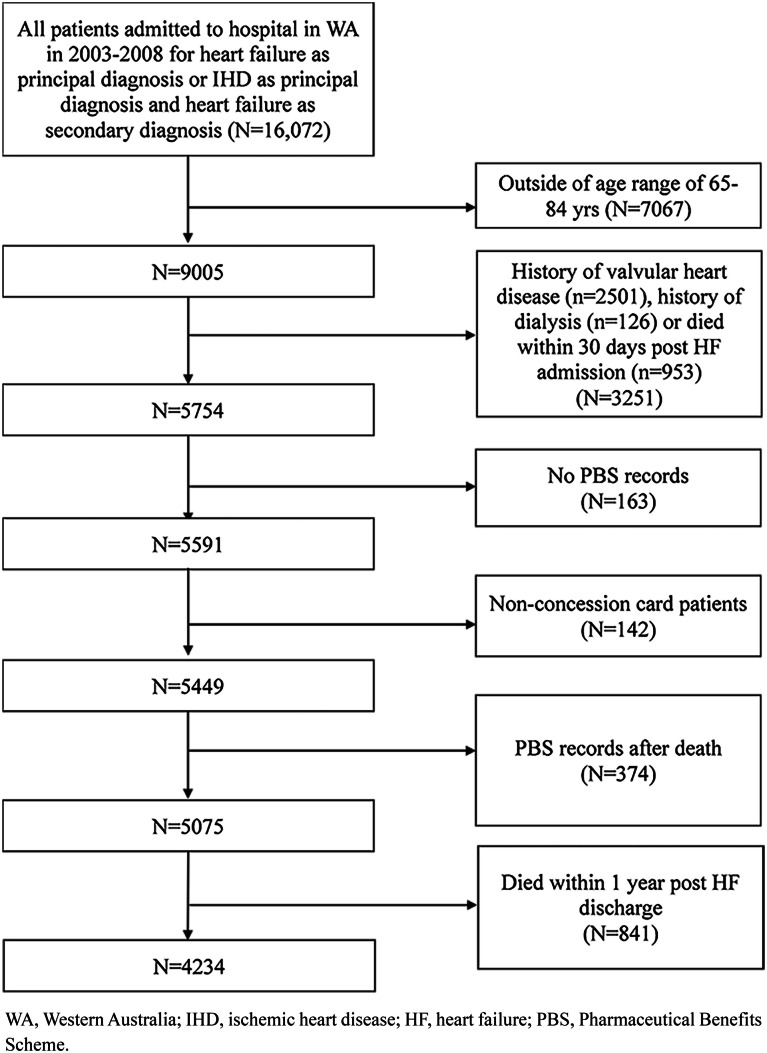
We identified a population-based cohort of 4234 patients, aged 65-84 years, 56% male, who were hospitalised for HF in Western Australia between 2003 and 2008 and survived to 1-year post-discharge (landmark date). Adherence was calculated using the proportion of days covered (PDC) in the first year post-discharge. RCS Cox proportional-hazards models were applied to determine the relationship between adherence and all-cause death and death/HF readmission at 1 and 3 years after the landmark date.
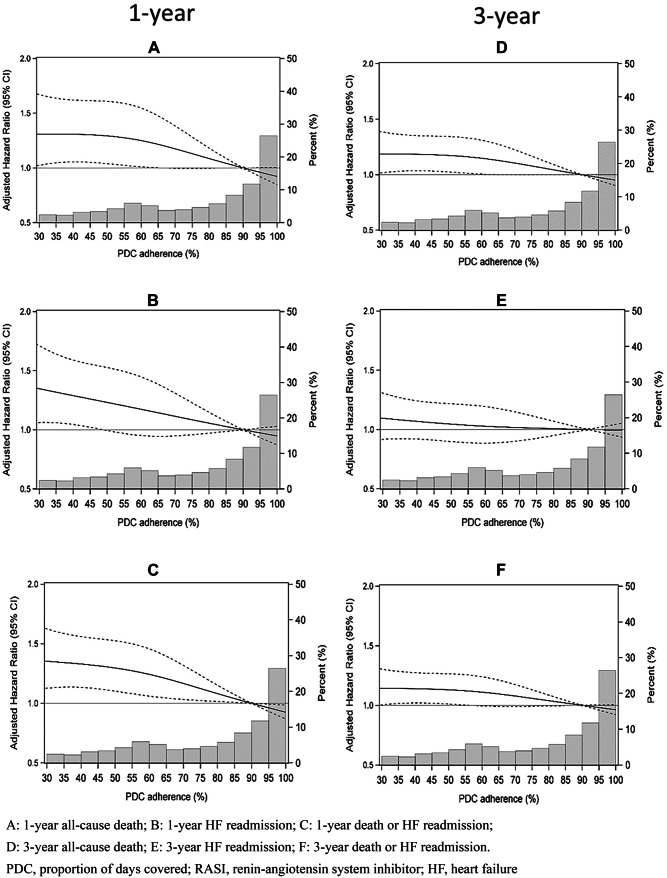
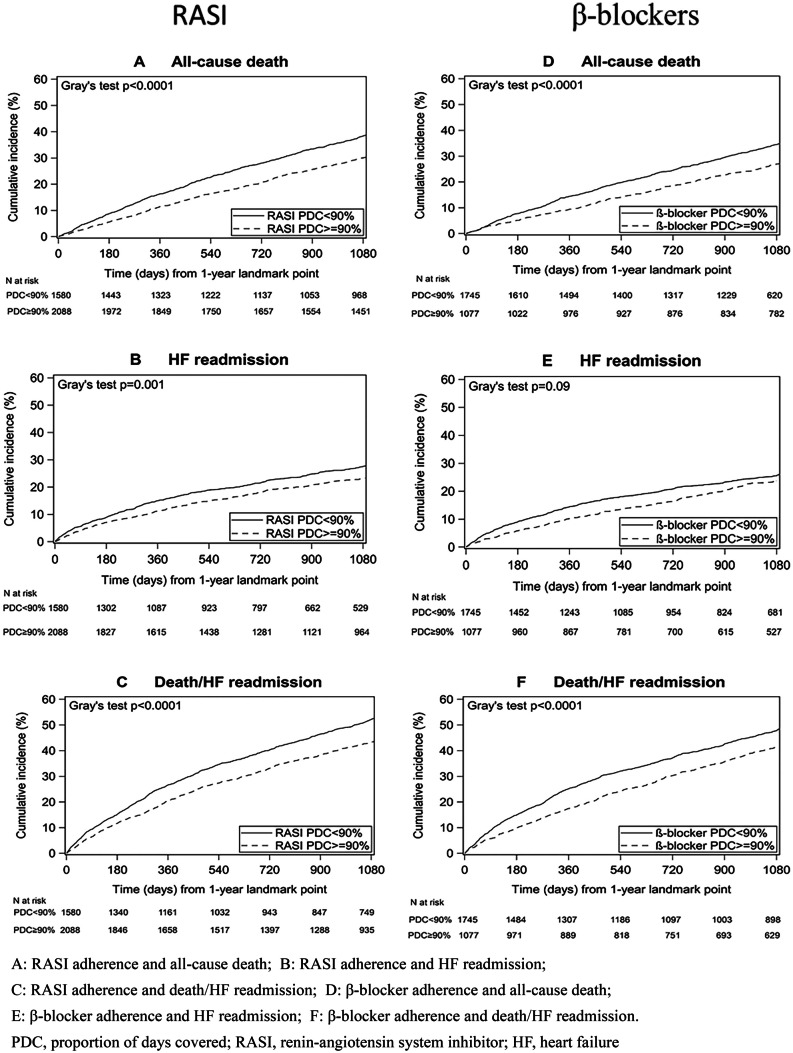
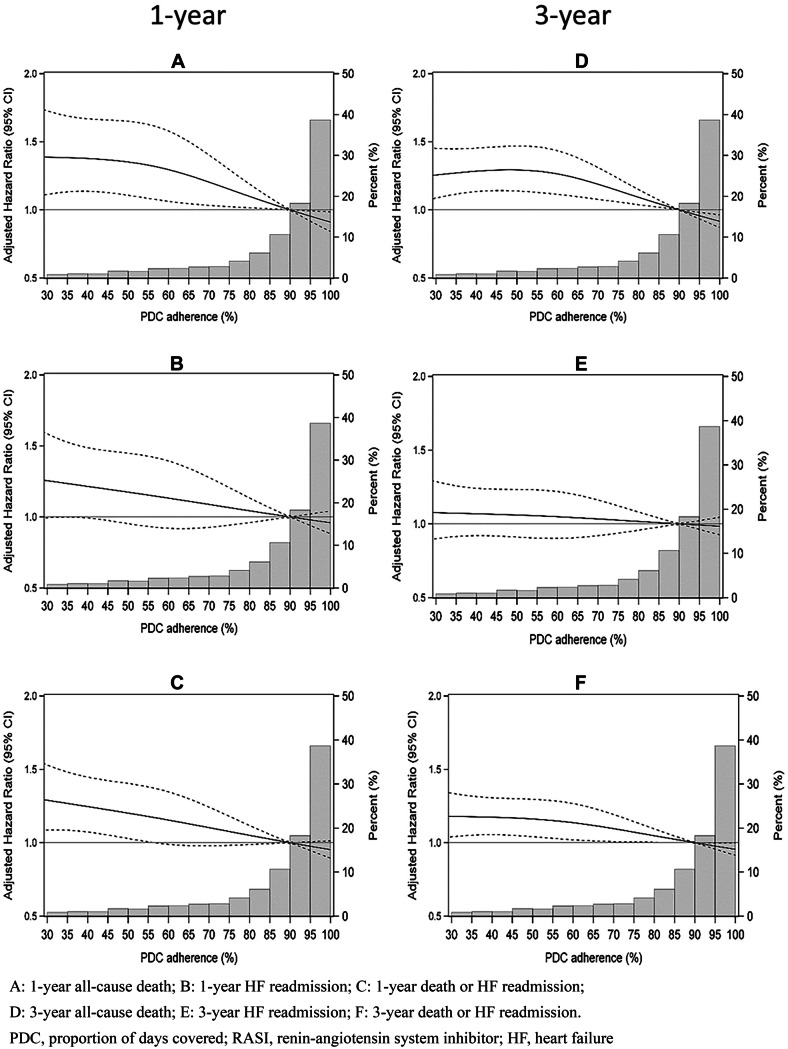
RCS analysis showed a curvilinear adherence-outcome relationship for both RASI and β-blockers which was linear above PDC 60%. For each 10% increase in RASI and β-blocker adherence above this level, the adjusted hazard ratio for 1-year all-cause death fell by an average of 6.6% and 4.8% respectively (trend p < 0.05) and risk of all-cause death/HF readmission fell by 5.4% and 5.8% respectively (trend p < 0.005). Linear reductions in adjusted risk for these outcomes at PDC ≥ 60% were also seen at 3 years after landmark date (all trend p < 0.05).
RCS analysis showed that for RASI and β-blockers, there was no upper adherence level (threshold) above 60% where risk reduction did not continue to occur. Therefore, interventions should maximise adherence to these disease-modifying HF pharmacotherapies to improve long-term outcomes after hospitalised HF.
心力衰竭(HF)药物治疗不依从与不良预后相关。我们使用限制三次样条(RCS)来评估老年 HF 患者药物治疗依从性与长期结局之间的连续关系。
我们确定了一个基于人群的队列,纳入了 4234 名年龄在 65-84 岁之间、56%为男性的患者,他们在 2003 年至 2008 年期间因 HF 在西澳大利亚住院治疗,并在出院后 1 年(标志日期)存活。依从性通过出院后第一年的比例日覆盖(PDC)来计算。应用限制三次样条 Cox 比例风险模型来确定依从性与标志日期后 1 年和 3 年时全因死亡和死亡/HF 再入院之间的关系。
RCS 分析显示,RASI 和β受体阻滞剂的依从性与结局之间呈曲线关系,在 PDC >60%时呈线性关系。在该水平之上,RASI 和β受体阻滞剂依从性每增加 10%,调整后的 1 年全因死亡风险平均降低 6.6%和 4.8%(趋势 p<0.05),全因死亡/HF 再入院风险分别降低 5.4%和 5.8%(趋势 p<0.005)。在标志日期后 3 年,PDC≥60%时也观察到这些结局的调整风险呈线性降低(所有趋势 p<0.05)。
RCS 分析表明,对于 RASI 和β受体阻滞剂,在 PDC>60%时,没有进一步提高依从性的上限(阈值)可以继续降低风险。因此,干预措施应最大程度地提高这些改善 HF 疾病的药物治疗的依从性,以改善住院 HF 后患者的长期结局。