Institut für Lungenbiologie (ILBD), Helmholtz Zentrum München, Deutsches Forschungszentrum für Gesundheit und Umwelt (GmbH), Ingolstädter Landstr. 1, 85764, München-Neuherberg, Germany.
Institut für KI und Informatik in der Medizin, Lehrstuhl für Medizinische Informatik, Klinikum rechts der Isar, Grillparzerstr. 18, 81675, München, Germany.
BMC Public Health. 2023 Mar 2;23(1):416. doi: 10.1186/s12889-023-15112-0.
During the first wave of the COVID-19 pandemic a high case fatality rate (CFR) was noticed worldwide including also Germany where the first European cases have been observed. The WHO recommended immediate intubation for patients with dyspnoea which has since been revised after reviewing the initial clinical outcome. The objective of this study is to analyze CFR and assess if there is an advantage of a more conservative management of COVID-19 induced hypoxemia.
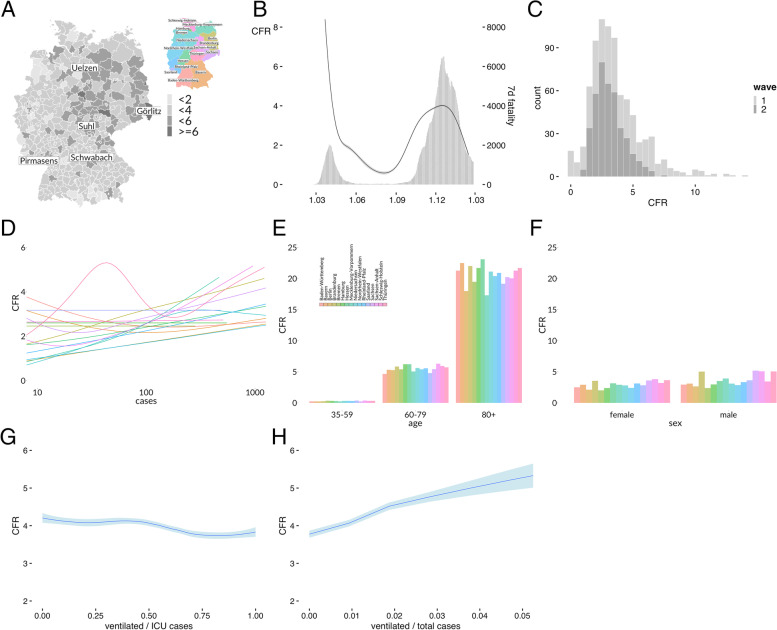
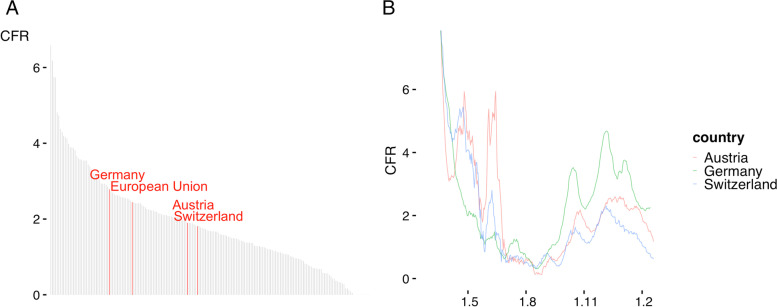
PCR confirmed COVID-19 infections and death counts were obtained for all German districts from 27 Jan 2020 until 15 Feb 2021 using official reports of Robert Koch Institute Berlin, Germany. A moving average CFRt was constructed by dividing disease related deaths two weeks after a given index day by the number of infections two weeks prior to that date. In addition to a local comparison also mortality outcomes in other German speaking countries were compared.
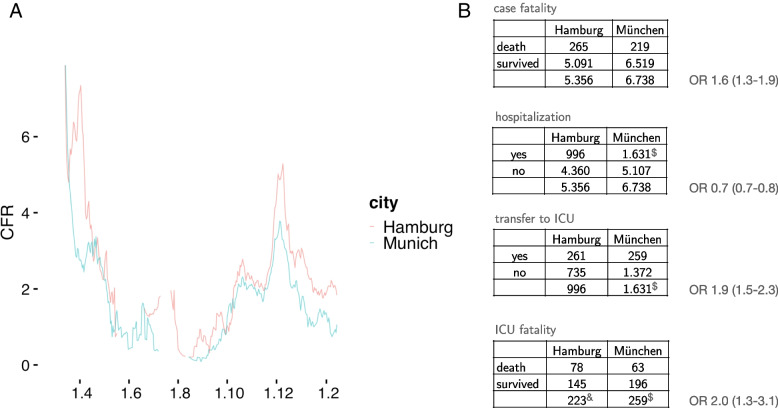
The mean CFR is estimated to be 2.92% based on 71.965 fatalities and 2.465.407 cases. There was a large regional scattering of CFRs across the German districts. Differences of the mortality pattern were observed also at state level and preserved across different sex and age groups while being largely independent of case numbers. Although Munich city had higher infection rates, more patients died during the first wave in Hamburg (OR 1.6, 95% CI 1.3-1.9) which was mirrored also by higher death risk at Hamburg intensive care units (OR 2.0, 95% CI 1.3-3.1). While the majority of Munich hospitals favoured a conservative management of hypoxemia including high flow nasal cannula (HFNC), Hamburg hospitals followed a more aggressive scheme of early mechanical ventilation (MV). Austria and Switzerland experienced higher CFRs than Germany during the first wave but after changing their treatment guidelines, both countries experienced lower CFRs during the second wave.
Using retrospective public health data, different case fatality rates have been observed across Germany. A more conservative management of COVID-19 induced Adult Respiratory Distress Syndrome (ARDS) is justified also by epidemiological data.
在 COVID-19 大流行的第一波期间,全球范围内的病死率(CFR)较高,包括德国,德国首次发现了欧洲病例。世界卫生组织建议对呼吸困难的患者立即进行插管,此后在审查了最初的临床结果后对该建议进行了修订。本研究的目的是分析病死率,并评估 COVID-19 引起的低氧血症更保守的治疗是否具有优势。
使用德国柏林罗伯特·科赫研究所的官方报告,从 2020 年 1 月 27 日至 2021 年 2 月 15 日,获得德国所有地区的 PCR 确诊 COVID-19 感染和死亡人数。通过将给定索引日后两周内与疾病相关的死亡人数除以该日期前两周内的感染人数,构建了一个移动平均 CFRt。除了进行本地比较外,还比较了其他德语国家的死亡率结果。
基于 71965 例死亡和 2465407 例病例,估计平均 CFR 为 2.92%。德国各地区的 CFR 存在很大的区域差异。在州一级也观察到死亡率模式的差异,并在不同性别和年龄组中保持一致,而基本独立于病例数量。尽管慕尼黑市的感染率较高,但汉堡市在第一波疫情中死亡的患者更多(OR 1.6,95%CI 1.3-1.9),这也反映在汉堡重症监护病房的死亡风险更高(OR 2.0,95%CI 1.3-3.1)。虽然大多数慕尼黑医院赞成对低氧血症进行保守治疗,包括高流量鼻导管(HFNC),但汉堡医院采用了早期机械通气(MV)的更激进方案。奥地利和瑞士在第一波疫情期间的病死率高于德国,但在改变治疗指南后,两国在第二波疫情期间的病死率均有所下降。
使用回顾性公共卫生数据,观察到德国各地的病死率不同。COVID-19 引起的成人呼吸窘迫综合征(ARDS)的更保守治疗也得到了流行病学数据的支持。