Department of Pediatrics, West China Second University Hospital, Sichuan University, Chengdu, China.
Ministry of Education Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Chengdu, China.
BMC Pediatr. 2023 Mar 2;23(1):100. doi: 10.1186/s12887-023-03917-2.
Hypochondroplasia (HCH) is a common nonlethal skeletal dysplasia caused by pathogenic variations in the fibroblast growth factor receptor 3 (FGFR3) gene, and HCH has similar clinical manifestations with achondroplasia (ACH), which can be screened during the fetal period by prenatal ultrasound testing and diagnosed by genetic testing.
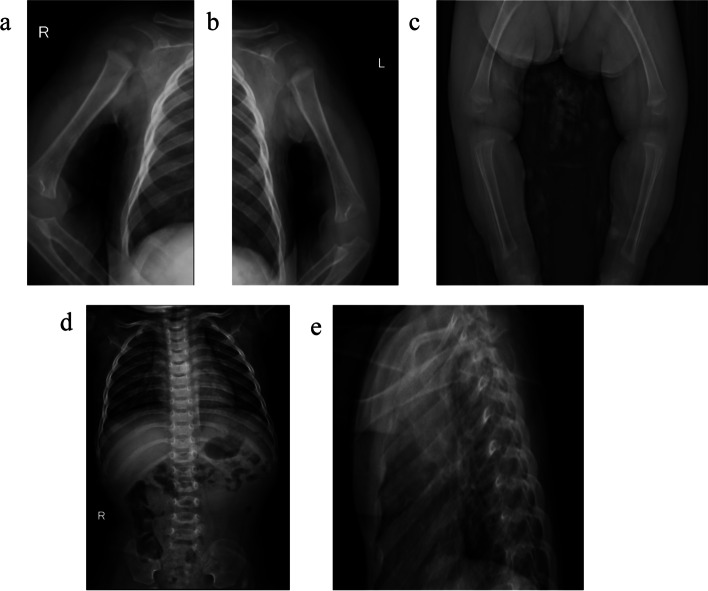
we report the special case of a patient with obvious growth retardation and rhizomelic disproportionate short stature, accompanied by other manifestations, including an enlarged head and short hands at 1 year old. However, several multiple color ultrasound exams identified shortened limbs (< 3rd percentile), an increased biparietal diameter (> 95th percentile) and a low nasal bridge in the fetal period. Due to the high incidence rate of ACH, genetic testing for the hotspot FGFR3 gene c.1138 g > A pathogenic variations was performed immediately in the third trimester. Unfortunately, the definitive diagnosis could not be made before birth due to the negative result of hotspot gene exam. Whole exome sequencing (WES) was performed at 1 year identified FGFR3 gene c.1620C > A variations positivity, and the patient was finally diagnosed as HCH.
Our report extends the understanding of the limitations of prenatal genetic diagnostic testing, especially the hot spot pathogenic variations test should be not the only clinical diagnostic basis. Moreover, this case also emphasizes that further gene analysis for patients with significant conflict between the clinical manifestation and the prenatal genetic panel examination findings should be reconducted timely to spare the family from a delayed diagnosis or a misdiagnosis.
软骨发育不全症(HCH)是一种常见的非致死性骨骼发育不良疾病,由成纤维细胞生长因子受体 3(FGFR3)基因的致病变异引起,HCH 与软骨发育不全症(ACH)具有相似的临床表现,可以通过产前超声检查在胎儿期进行筛查,并通过基因检测进行诊断。
我们报告了一名患者的特殊病例,该患者存在明显的生长迟缓、四肢骨干短、四肢不成比例,伴有其他表现,包括头部增大和手部短。然而,几次多次彩色超声检查在胎儿期识别出四肢缩短(<第 3 百分位)、双额直径增加(>第 95 百分位)和鼻梁低。由于 ACH 的发病率高,立即在妊娠晚期对热点 FGFR3 基因 c.1138g> A 致病变异进行了基因检测。不幸的是,由于热点基因检测结果为阴性,出生前无法做出明确诊断。在 1 岁时进行全外显子组测序(WES)发现 FGFR3 基因 c.1620C> A 变异阳性,最终诊断为 HCH。
我们的报告扩展了对产前遗传诊断检测局限性的认识,特别是热点致病变异检测不应是唯一的临床诊断依据。此外,该病例还强调,对于临床表现与产前基因panel 检查结果明显冲突的患者,应及时重新进行基因分析,以免家庭面临诊断延迟或误诊。