Vigotti Federica N, Di Benedetto Carlo, Fop Fabrizio, Bianco Simona, Bilucaglia Donatella, Cesano Giulio
Nephrology and Dialysis, Martini Hospital, ASL Città di Torino, Turin, Italy.
University of Turin, Nephrology and Dialysis, San Giovanni Bosco Hospital, ASL Città di Torino, Turin, Italy.
Clin Kidney J. 2022 Dec 16;16(3):541-548. doi: 10.1093/ckj/sfac250. eCollection 2023 Mar.
Interest in point-of-care ultrasound (POCUS) and lung ultrasound (LUS) is growing in the nephrology and dialysis field, and the number of nephrologists skilled in what is proving to be the "5th pillar of bedside physical examination" is increasing. Patients on hemodialysis (HD) are at high risk of contracting severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) and developing coronavirus disease 2019 (COVID-19) serious complications. Despite this, to our knowledge there are no studies to date that show the role of LUS in this setting, while there are many in the emergency room, where LUS proved to be an important tool, providing risk stratification and guiding management strategies and resource allocation. Therefore, it is not clear whether the usefulness and cut-offs of LUS highlighted in studies in the general population are reliable in dialysis, or whether variations, precautions and adjustments to this specific situation are necessary.
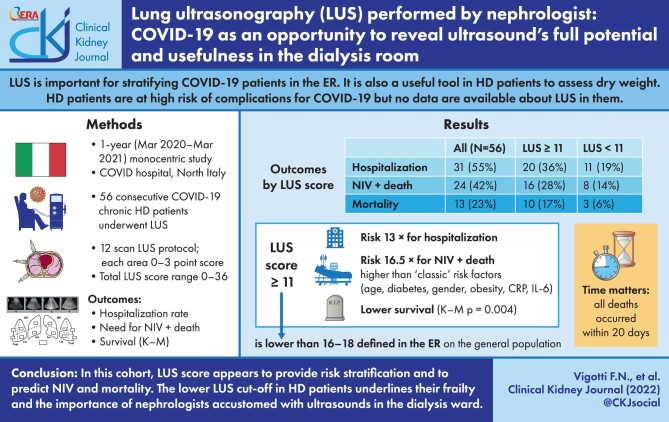
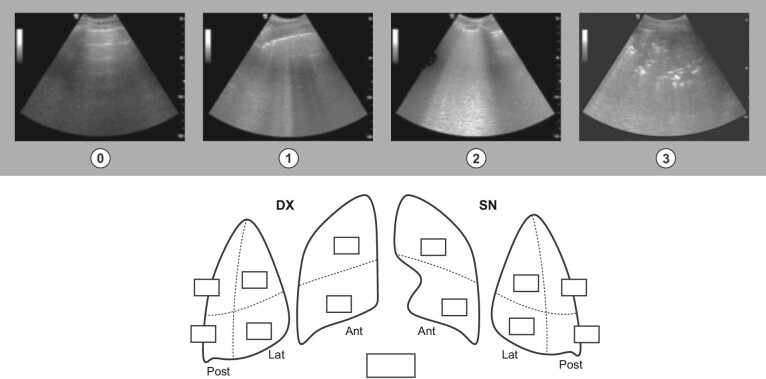
This was a 1-year monocentric prospective observational cohort study of 56 HD patients with COVID-19. Patients underwent a monitoring protocol that included at first evaluation bedside LUS, using a 12-scan scoring system, by the same nephrologist. All data were prospectively and systematically collected. Outcomes. hospitalization rate, combined outcome [non-invasive ventilation (NIV + death)], mortality. Descriptive variables are presented as medians (interquartile range), or percentage. Univariate and multivariate analysis, as well as Kaplan-Meier (K-M) survival curves, were carried out. was fixed at .05.
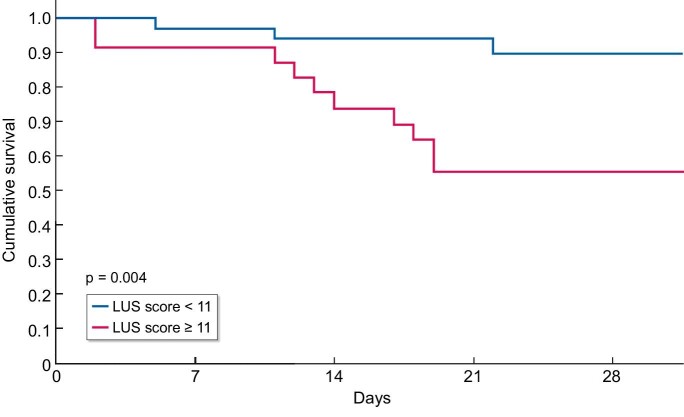
Median age was 78 years, 90% had at least one comorbidity (46% diabetics), 55% were hospitalized and 23% deaths. Median duration of disease was 23 days (14-34). A LUS score ≥11 represented a 13-fold risk of hospitalization, a 16.5-fold risk of combined outcome (NIV + death) vs risk factors such as age [odds ratio (OR) 1.6], diabetes (OR 1.2), male sex (OR 1.3) and obesity (OR 1.25), and a 7.7-fold risk of mortality. In the logistic regression, LUS score ≥11 is associated with the combined outcome with a hazard ratio (HR) of 6.1 vs inflammations indices such as CRP ≥9 mg/dL (HR 5.5) and interleukin-6 (IL-6) ≥62 pg/mL (HR 5.4). In K-M curves, survival drops significantly with LUS score above 11.
In our experience of COVID-19 HD patients, LUS appeared to be an effective and easy tool, predicting the need for NIV and mortality better than "classic" known COVID-19 risk factors such as age, diabetes, male sex and obesity, and even better than inflammations indices such as CRP and IL-6. These results are consistent with those of the studies in the emergency room setting, but with a lower LUS score cut-off (11 vs 16-18). This is probably due to the higher global frailty and peculiarity of HD population, and emphasizes how nephrologists should themselves use LUS and POCUS as a part of their everyday clinical practice, adapting it to the peculiarity of the HD ward.
在肾脏病学和透析领域,对床旁超声(POCUS)和肺部超声(LUS)的关注日益增加,并且熟练掌握这一被证明是“床旁体格检查第五支柱”技能的肾脏病专家数量也在增多。接受血液透析(HD)的患者感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)并发展为2019冠状病毒病(COVID-19)严重并发症的风险很高。尽管如此,据我们所知,目前尚无研究表明LUS在此情况下的作用,而在急诊室有许多相关研究,在那里LUS被证明是一种重要工具,可提供风险分层并指导管理策略和资源分配。因此,尚不清楚在普通人群研究中所强调的LUS的有用性和临界值在透析患者中是否可靠,或者是否需要针对这种特殊情况进行变异、预防措施和调整。
这是一项对56例COVID-19血液透析患者进行的为期1年的单中心前瞻性观察队列研究。患者接受了一项监测方案,在首次评估时由同一位肾脏病专家使用12项扫描评分系统进行床旁LUS检查。所有数据均进行前瞻性和系统性收集。观察指标:住院率、综合结局[无创通气(NIV +死亡)]、死亡率。描述性变量以中位数(四分位间距)或百分比表示。进行单因素和多因素分析以及Kaplan-Meier(K-M)生存曲线分析。P值设定为0.05。
中位年龄为78岁,90%的患者至少有一种合并症(46%为糖尿病患者),55%的患者住院,23%的患者死亡。疾病中位持续时间为23天(14 - 34天)。LUS评分≥11表示住院风险是年龄[比值比(OR)1.6]、糖尿病(OR 1.2)、男性(OR 1.3)和肥胖(OR 1.25)等风险因素的13倍,综合结局(NIV +死亡)风险的16.5倍,以及死亡风险的7.7倍。在逻辑回归中,LUS评分≥11与综合结局相关,风险比(HR)为6.1,而与炎症指标如C反应蛋白(CRP)≥9 mg/dL(HR 5.5)和白细胞介素-6(IL-6)≥62 pg/mL(HR 5.4)相比。在K-M曲线中,LUS评分高于11时生存率显著下降。
根据我们对COVID-19血液透析患者的经验,LUS似乎是一种有效且简便的工具,比年龄、糖尿病、男性和肥胖等“经典”已知COVID-19风险因素,甚至比CRP和IL-6等炎症指标,能更好地预测无创通气需求和死亡率。这些结果与急诊室环境中的研究结果一致,但LUS评分临界值更低(11对比16 - 18)。这可能是由于血液透析人群总体虚弱程度更高和特殊性所致,并强调肾脏病专家应将LUS和POCUS作为日常临床实践的一部分,使其适应血液透析病房的特殊性。