Noparatkailas Nabhat, Inchai Juthamas, Deesomchok Athavudh
Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, Muang, Chiang Mai, Thailand.
Indian J Crit Care Med. 2023 Feb;27(2):93-100. doi: 10.5005/jp-journals-10071-24404.
To evaluate the association of initial blood lactate with mortality and subsequent septic shock in non-shock septic patients.
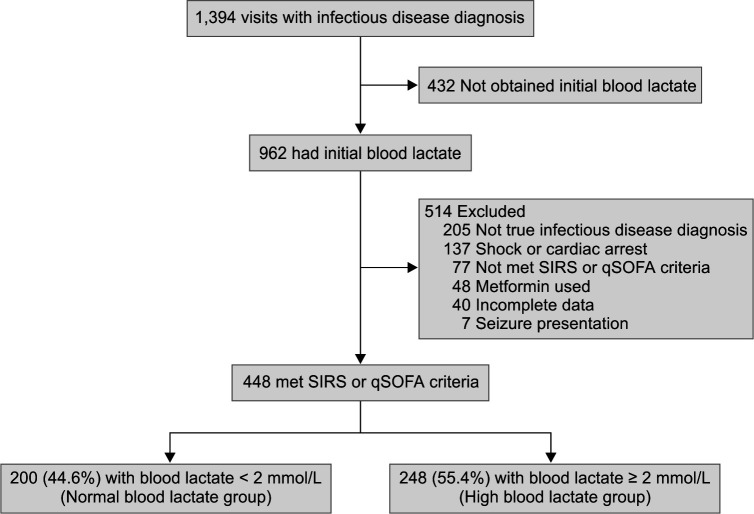
A retrospective cohort study was conducted at Maharaj Nakorn Chiang Mai Hospital, Chiang Mai University, Muang, Chiang Mai, Thailand. Inclusion criteria included septic patients admitted to a non-critical medical ward and had initial serum lactate at the emergency department (ED). Shock and other causes of hyperlactatemia were excluded.
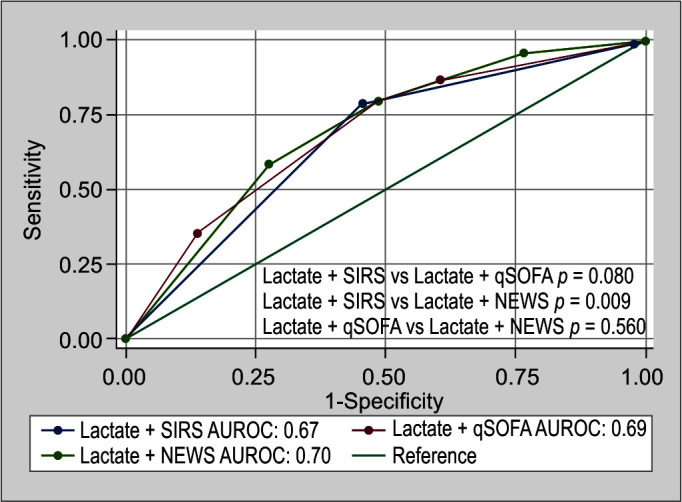
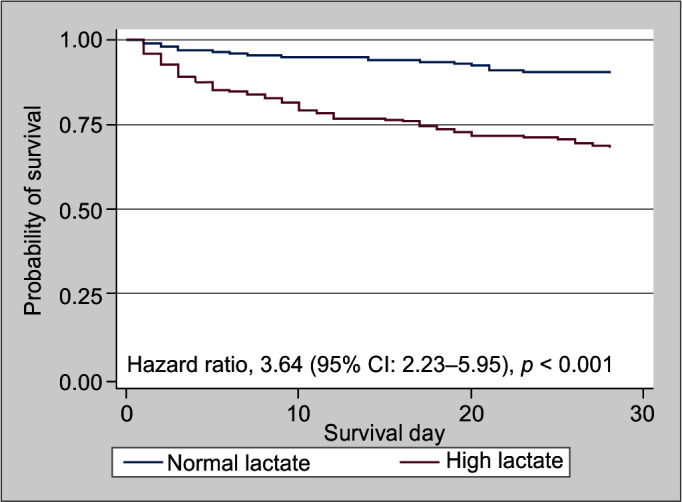
A total of 448 admissions were included with median age [interquartile range (IQR)] of 71 (59, 87) years and 200 males (44.6%). Pneumonia was the most common cause of sepsis (47.5%). The median systemic inflammatory response syndrome (SIRS) and quick sequential organ failure assessment (qSOFA) scores were 3 (2, 3) and 1 (1, 2), respectively. The median initial blood lactate was 2.19 (1.45, 3.23) mmol/L. The high blood lactate (≥2 mmol/L) group; = 248, had higher qSOFA and other predictive scores and had significantly higher 28 days mortality (31.9% vs 10.0%; < 0.001) and subsequent 3 days septic shock (18.1% vs 5.0%; < 0.001) than the normal blood lactate group; = 200. A combination of blood lactate above or equal to 2 mmol/L plus the national early warning score (NEWS) above or equal to 7 showed the highest prediction of 28 days mortality with the area under receiver-operating characteristic curve (AUROC) of 0.70 [95% confidence interval (CI): 0.65-0.75].
An initial blood lactate level above or equal to 2 mmol/L is associated with high mortality and subsequent septic shock among non-shock septic patients. The composite of blood lactate levels and other predictive scores yields better accuracy to predict mortality.
Noparatkailas N, Inchai J, Deesomchok A. Blood Lactate Level and the Predictor of Death in Non-shock Septic Patients. Indian J Crit Care Med 2023;27(2):93-100.
评估非休克型脓毒症患者初始血乳酸水平与死亡率及随后发生感染性休克的相关性。
在泰国清迈府清迈市清迈大学玛哈叻那空清迈医院进行了一项回顾性队列研究。纳入标准包括入住非重症内科病房且在急诊科有初始血清乳酸水平的脓毒症患者。排除休克及其他高乳酸血症原因。
共纳入448例患者,中位年龄[四分位间距(IQR)]为71(59,87)岁,男性200例(44.6%)。肺炎是脓毒症最常见的病因(47.5%)。全身炎症反应综合征(SIRS)和快速序贯器官衰竭评估(qSOFA)评分的中位数分别为3(2,3)和1(1,2)。初始血乳酸水平的中位数为2.19(1.45,3.23)mmol/L。高血乳酸(≥2 mmol/L)组(n = 248)的qSOFA及其他预测评分更高,28天死亡率(31.9%对10.0%;P < 0.001)和随后3天发生感染性休克的比例(18.1%对5.0%;P < 0.001)均显著高于正常血乳酸组(n = 200)。血乳酸水平高于或等于2 mmol/L加上国家早期预警评分(NEWS)高于或等于7对28天死亡率的预测能力最强,受试者工作特征曲线下面积(AUROC)为0.70[95%置信区间(CI):0.65 - 0.75]。
非休克型脓毒症患者初始血乳酸水平高于或等于2 mmol/L与高死亡率及随后发生感染性休克相关。血乳酸水平与其他预测评分的综合可提高预测死亡率的准确性。
Noparatkailas N, Inchai J, Deesomchok A. 非休克型脓毒症患者的血乳酸水平与死亡预测因素。《印度重症监护医学杂志》2023;27(2):93 - 100。