Mehra Niven, Kloots Iris, Vlaming Michiel, Aluwini Shafak, Dewulf Els, Oprea-Lager Daniela E, van der Poel Henk, Stoevelaar Herman, Yakar Derya, Bangma Chris H, Bekers Elise, van den Bergh Roderick, Bergman Andries M, van den Berkmortel Franchette, Boudewijns Steve, Dinjens Winand N M, Fütterer Jurgen, van der Hulle Tom, Jenster Guido, Kroeze Leonie I, van Kruchten Michel, van Leenders Geert, van Leeuwen Pim J, de Leng Wendy W J, van Moorselaar R Jeroen A, Noordzij Walter, Oldenburg Rogier A, van Oort Inge M, Oving Irma, Schalken Jack A, Schoots Ivo G, Schuuring Ed, Smeenk Robert J, Vanneste Ben G L, Vegt Erik, Vis André N, de Vries Kim, Willemse Peter-Paul M, Wondergem Maurits, Ausems Margreet
Department of Medical Oncology, Radboud UMC, Nijmegen, The Netherlands.
Division Laboratories, Pharmacy and biomedical Genetics, Department of Genetics, University Medical Centre Utrecht, Utrecht, The Netherlands.
Eur Urol Open Sci. 2023 Jan 25;49:23-31. doi: 10.1016/j.euros.2022.11.011. eCollection 2023 Mar.
Germline and tumour genetic testing in prostate cancer (PCa) is becoming more broadly accepted, but testing indications and clinical consequences for carriers in each disease stage are not yet well defined.
To determine the consensus of a Dutch multidisciplinary expert panel on the indication and application of germline and tumour genetic testing in PCa.
The panel consisted of 39 specialists involved in PCa management. We used a modified Delphi method consisting of two voting rounds and a virtual consensus meeting.
Consensus was reached if ≥75% of the panellists chose the same option. Appropriateness was assessed by the RAND/UCLA appropriateness method.
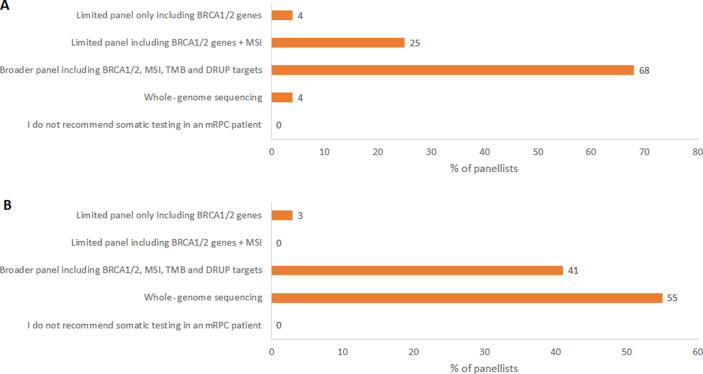
Of the multiple-choice questions, 44% reached consensus. For men without PCa having a relevant family history (familial PCa/-related hereditary cancer), follow-up by prostate-specific antigen was considered appropriate. For patients with low-risk localised PCa and a family history of PCa, active surveillance was considered appropriate, except in case of the patient being a germline pathogenic variant carrier. Germline and tumour genetic testing should not be done for nonmetastatic hormone-sensitive PCa in the absence of a relevant family history of cancer. Tumour genetic testing was deemed most appropriate for the identification of actionable variants, with uncertainty for germline testing. For tumour genetic testing in metastatic castration-resistant PCa, consensus was not reached for the timing and panel composition. The principal limitations are as follows: (1) a number of topics discussed lack scientific evidence, and therefore the recommendations are partly opinion based, and (2) there was a small number of experts per discipline.
The outcomes of this Dutch consensus meeting may provide further guidance on genetic counselling and molecular testing related to PCa.
A group of Dutch specialists discussed the use of germline and tumour genetic testing in prostate cancer (PCa) patients, indication of these tests (which patients and when), and impact of these tests on the management and treatment of PCa.
前列腺癌(PCa)的种系和肿瘤基因检测正越来越被广泛接受,但每种疾病阶段携带者的检测指征和临床后果尚未明确界定。
确定荷兰多学科专家小组对PCa种系和肿瘤基因检测的指征及应用的共识。
设计、设置和参与者:该小组由39名参与PCa管理的专家组成。我们采用了一种改良的德尔菲法,包括两轮投票和一次虚拟共识会议。
如果≥75%的小组成员选择相同选项,则达成共识。适宜性通过RAND/UCLA适宜性方法进行评估。
在多项选择题中,44%达成了共识。对于没有PCa但有相关家族史(家族性PCa/相关遗传性癌症)的男性,通过前列腺特异性抗原进行随访被认为是合适的。对于低风险局限性PCa且有PCa家族史的患者,除患者是种系致病变异携带者外,主动监测被认为是合适的。在没有相关癌症家族史的情况下,不应为非转移性激素敏感性PCa进行种系和肿瘤基因检测。肿瘤基因检测被认为最适合于识别可操作的变异,种系检测存在不确定性。对于转移性去势抵抗性PCa的肿瘤基因检测,在检测时间和检测组组成方面未达成共识。主要局限性如下:(1)讨论的一些主题缺乏科学证据,因此建议部分基于观点;(2)每个学科的专家数量较少。
本次荷兰共识会议的结果可能为与PCa相关的遗传咨询和分子检测提供进一步指导。
一组荷兰专家讨论了前列腺癌(PCa)患者种系和肿瘤基因检测的使用、这些检测的指征(哪些患者以及何时进行)以及这些检测对PCa管理和治疗的影响。