Piquette Dominique, Burns Karen E A, Carnevale Franco, Sarti Aimée J, Hamilton Mika, Dodek Peter M
Department of Critical Care Medicine, Sunnybrook Health Sciences Centre, Toronto, ON, Canada.
Inter-Departmental Division of Critical Care Medicine, University of Toronto, Toronto, ON, Canada.
Crit Care Explor. 2023 Mar 6;5(3):e0879. doi: 10.1097/CCE.0000000000000879. eCollection 2023 Mar.
Moral distress is common among critical care physicians and can impact negatively healthcare individuals and institutions. Better understanding inter-individual variability in moral distress is needed to inform future wellness interventions.
To explore when and how critical care physicians experience moral distress in the workplace and its consequences, how physicians' professional interactions with colleagues affected their perceived level of moral distress, and in which circumstances professional rewards were experienced and mitigated moral distress.
Interview-based qualitative study using inductive thematic analysis.
Twenty critical care physicians practicing in Canadian ICUs who expressed interest in participating in a semi-structured interview after completion of a national, cross-sectional survey of moral distress in ICU physicians.
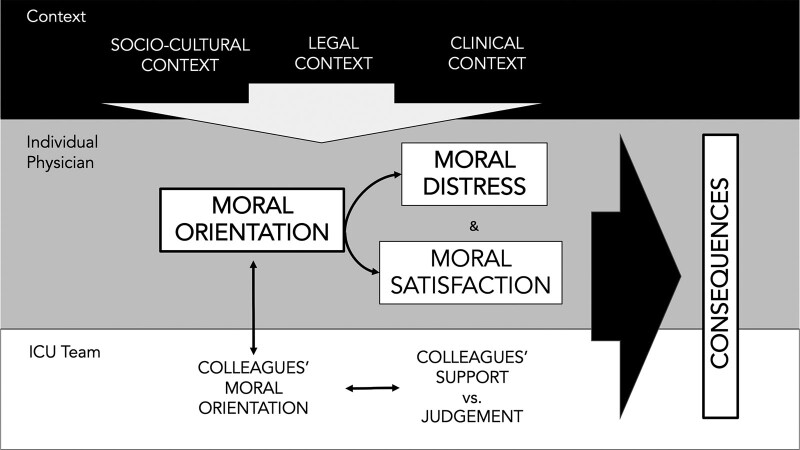
Study participants described different ways to perceive and resolve morally challenging clinical situations, which were grouped into four clinical moral orientations: virtuous, resigned, deferring, and empathic. Moral orientations resulted from unique combinations of strength of personal moral beliefs and perceived power over moral clinical decision-making, which led to different rationales for moral decision-making. Study findings illustrate how sociocultural, legal, and clinical contexts influenced individual physicians' moral orientation and how moral orientation altered perceived moral distress and moral satisfaction. The degree of dissonance between individual moral orientations within care team determined, in part, the quantity of "negative judgments" and/or "social support" that physicians obtained from their colleagues. The levels of moral distress, moral satisfaction, social judgment, and social support ultimately affected the type and severity of the negative consequences experienced by ICU physicians.
An expanded understanding of moral orientations provides an additional tool to address the problem of moral distress in the critical care setting. Diversity in moral orientations may explain, in part, the variability in moral distress levels among clinicians and likely contributes to interpersonal conflicts in the ICU setting. Additional investigations on different moral orientations in various clinical environments are much needed to inform the design of effective systemic and institutional interventions that address healthcare professionals' moral distress and mitigate its negative consequences.
道德困扰在重症监护医生中很常见,会对医护人员个体和机构产生负面影响。需要更好地了解道德困扰的个体间差异,为未来的健康干预提供依据。
探讨重症监护医生在工作场所何时以及如何经历道德困扰及其后果,医生与同事的专业互动如何影响他们感知到的道德困扰程度,以及在哪些情况下会体验到职业回报并减轻道德困扰。
基于访谈的定性研究,采用归纳主题分析。
20名在加拿大重症监护病房工作的重症监护医生,他们在完成一项关于重症监护病房医生道德困扰的全国性横断面调查后,表示有兴趣参加半结构式访谈。
研究参与者描述了感知和解决道德挑战性临床情况的不同方式,这些方式被归纳为四种临床道德取向:高尚、顺从、 deferring(此处原文可能有误,暂按原样翻译)、共情。道德取向源于个人道德信念的强度和对道德临床决策的感知权力的独特组合,这导致了道德决策的不同理由。研究结果说明了社会文化、法律和临床背景如何影响个体医生的道德取向,以及道德取向如何改变感知到的道德困扰和道德满意度。护理团队中个体道德取向之间的不一致程度部分决定了医生从同事那里获得的“负面评价”和/或“社会支持”的数量。道德困扰、道德满意度、社会评判和社会支持的水平最终影响了重症监护医生所经历的负面后果的类型和严重程度。
对道德取向的更广泛理解为解决重症监护环境中的道德困扰问题提供了一个额外的工具。道德取向的多样性可能部分解释了临床医生道德困扰水平的差异,并可能导致重症监护环境中的人际冲突。迫切需要在各种临床环境中对不同的道德取向进行更多调查,以为设计有效的系统和机构干预措施提供依据,这些干预措施旨在解决医护人员的道德困扰并减轻其负面后果。