Department of Accounting Information, Chihlee University of Technology, Taipei 22050, Taiwan.
Graduate Institute of Business Administration, College of Management, Fu Jen Catholic University, Taipei 24205, Taiwan.
Nutrients. 2023 Mar 1;15(5):1247. doi: 10.3390/nu15051247.
The relationship between the onset of sarcopenia prior to cancer diagnosis and survival outcomes in various types of cancer is not well understood. To address this gap in knowledge, we conducted a propensity score-matched population-based cohort study to compare the overall survival of cancer patients with and without sarcopenia.
In our study, we included patients with cancer and divided them into two groups based on the presence or absence of sarcopenia. To ensure comparability between the groups, we matched patients in both groups at a ratio of 1:1.
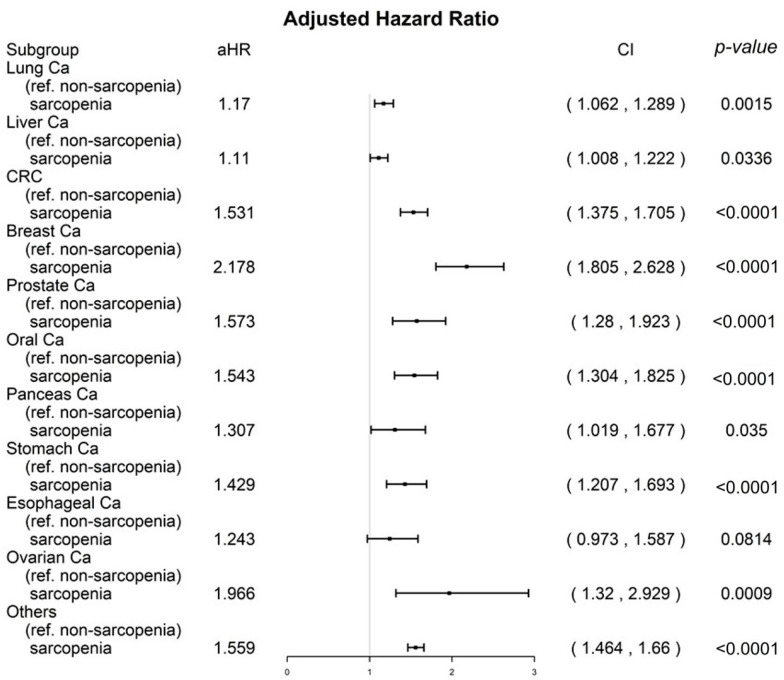
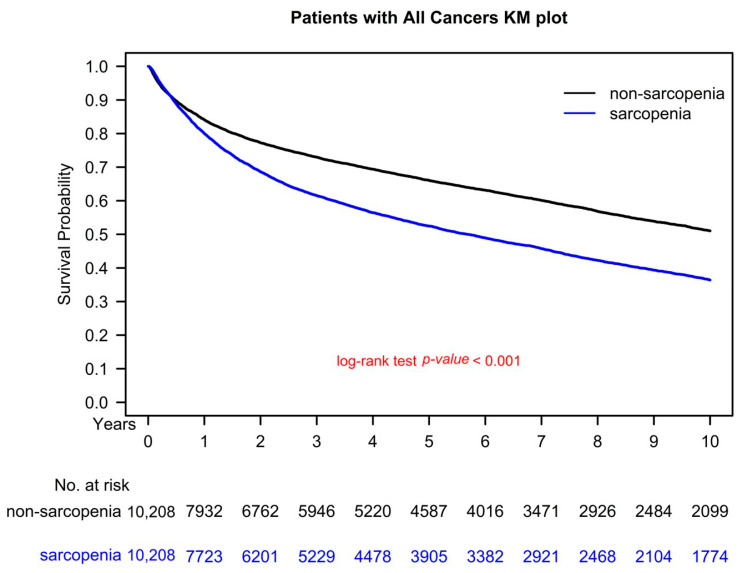
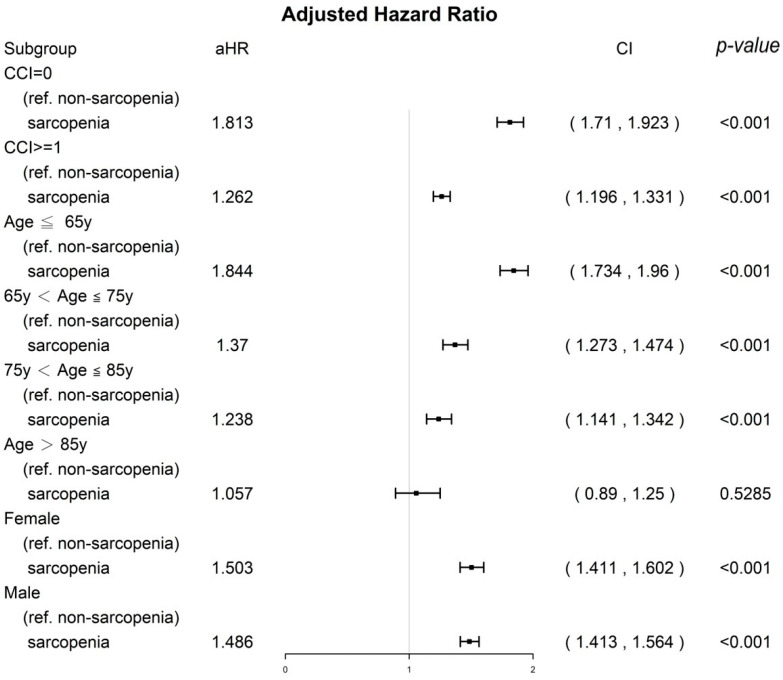
After the matching process, our final cohort included 20,416 patients with cancer (10,208 in each group) who were eligible for further analysis. There were no significant differences between the sarcopenia and nonsarcopenia groups in terms of confounding factors such as age (mean 61.05 years versus 62.17 years), gender (52.56% versus 52.16% male, 47.44% versus 47.84% female), comorbidities, and cancer stages. In our multivariate Cox regression analysis, we found that the adjusted hazard ratio (aHR; 95% confidence interval [CI]) of all-cause death for the sarcopenia group compared to the nonsarcopenia group was 1.49 (1.43-1.55; < 0.001). Additionally, the aHRs (95% CIs) of all-cause death for those aged 66-75, 76-85, and >85 years (compared to those aged ≤65 years) were 1.29 (1.23-1.36), 2.00 (1.89-2.12), and 3.26 (2.97-3.59), respectively. The aHR (95% CI) of all-cause death for those with a Charlson comorbidity index (CCI) ≥ 1 compared to those with a CCI of 0 was 1.34 (1.28-1.40). The aHR (95% CI) of all-cause death for men compared to women was 1.56 (1.50-1.62). When comparing the sarcopenia and nonsarcopenia groups, the aHRs (95% CIs) for lung, liver, colorectal, breast, prostate, oral, pancreatic, stomach, ovarian, and other cancers were significantly higher.
Our findings suggest that the onset of sarcopenia prior to cancer diagnosis may be linked to reduced survival outcomes in cancer patients.
癌症诊断前发生的肌肉减少症与各种类型癌症的生存结局之间的关系尚未得到充分了解。为了弥补这一知识空白,我们进行了一项倾向评分匹配的基于人群的队列研究,比较了有和无肌肉减少症的癌症患者的总生存率。
在我们的研究中,我们纳入了患有癌症的患者,并根据是否存在肌肉减少症将他们分为两组。为了确保两组之间的可比性,我们以 1:1 的比例对两组患者进行了匹配。
在匹配过程之后,我们的最终队列包括 20416 名癌症患者(每组 10208 名),他们符合进一步分析的条件。在年龄(平均 61.05 岁对 62.17 岁)、性别(52.56%对男性,47.44%对女性)、合并症和癌症分期等混杂因素方面,肌肉减少症组和非肌肉减少症组之间没有显著差异。在我们的多变量 Cox 回归分析中,我们发现与非肌肉减少症组相比,肌肉减少症组的全因死亡调整后的危险比(aHR;95%置信区间[CI])为 1.49(1.43-1.55;<0.001)。此外,年龄在 66-75 岁、76-85 岁和>85 岁的患者(与年龄≤65 岁的患者相比)的全因死亡的 aHR(95%CI)分别为 1.29(1.23-1.36)、2.00(1.89-2.12)和 3.26(2.97-3.59)。与Charlson 合并症指数(CCI)为 0 的患者相比,CCI≥1 的患者的全因死亡的 aHR(95%CI)为 1.34(1.28-1.40)。与女性相比,男性的全因死亡的 aHR(95%CI)为 1.56(1.50-1.62)。与非肌肉减少症组相比,患有肺癌、肝癌、结直肠癌、乳腺癌、前列腺癌、口腔癌、胰腺癌、胃癌、卵巢癌和其他癌症的患者的 aHR(95%CI)显著更高。
我们的研究结果表明,癌症诊断前发生的肌肉减少症可能与癌症患者的生存结局降低有关。