Sparano Clotilde, Adornato Virginia, Puccioni Matteo, Zago Elena, Perigli Giuliano, Badii Benedetta, Santoro Roberto, Maggi Mario, Petrone Luisa
Endocrinology Unit, Department of Experimental and Clinical Biomedical Sciences 'Mario Serio', University of Florence, Florence, Italy.
Unit of General and Endocrine Surgery, Centre of Oncological and Minimally Invasive Surgery, Department of Surgery and Translational Medicine, University of Florence, Florence, Italy.
Front Oncol. 2023 Feb 24;13:1120799. doi: 10.3389/fonc.2023.1120799. eCollection 2023.
Calcitonin is the most specific marker for medullary thyroid carcinoma, thus, low detectable calcitonin values after surgery can conceal persistent disease. The present study aimed to explore the prognostic role of pre-operative and calcitonin levels in patients without distant metastases at diagnosis.
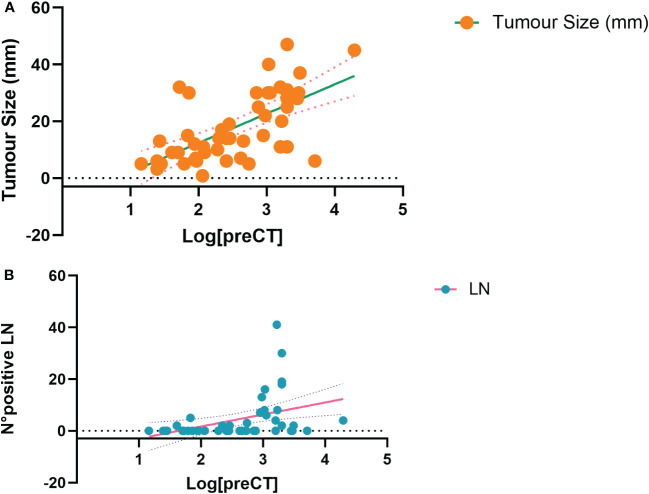
A retrospective cohort of patients suffering from medullary thyroid carcinoma was considered (N=55). The final disease status, i.e. (undetectable calcitonin levels and negative radiological assessments) or (detectable calcitonin levels and/or positive radiological assessments), was deduced from the last available follow-up. Pre-operative and calcitonin levels (i.e. six months after surgery) have been correlated to several clinical and histological features, according to the final disease status.
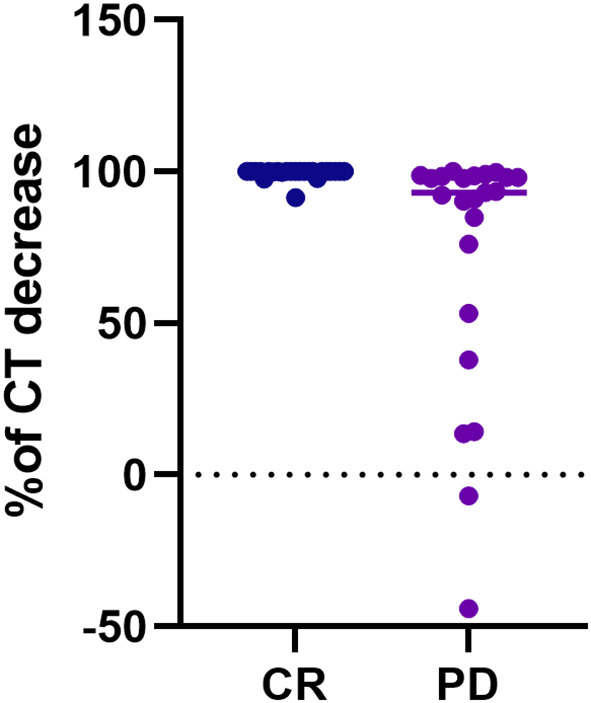
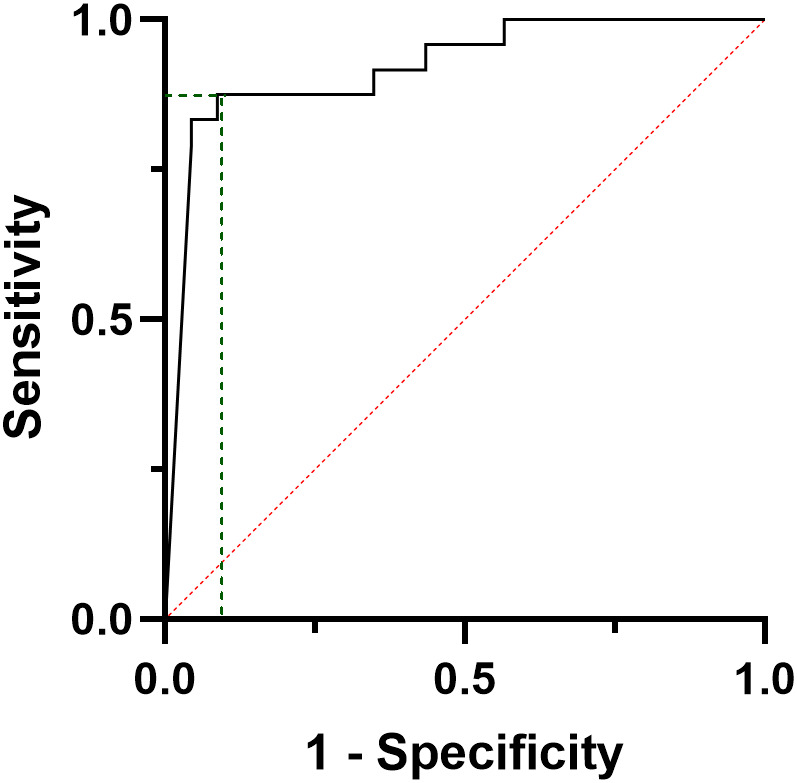
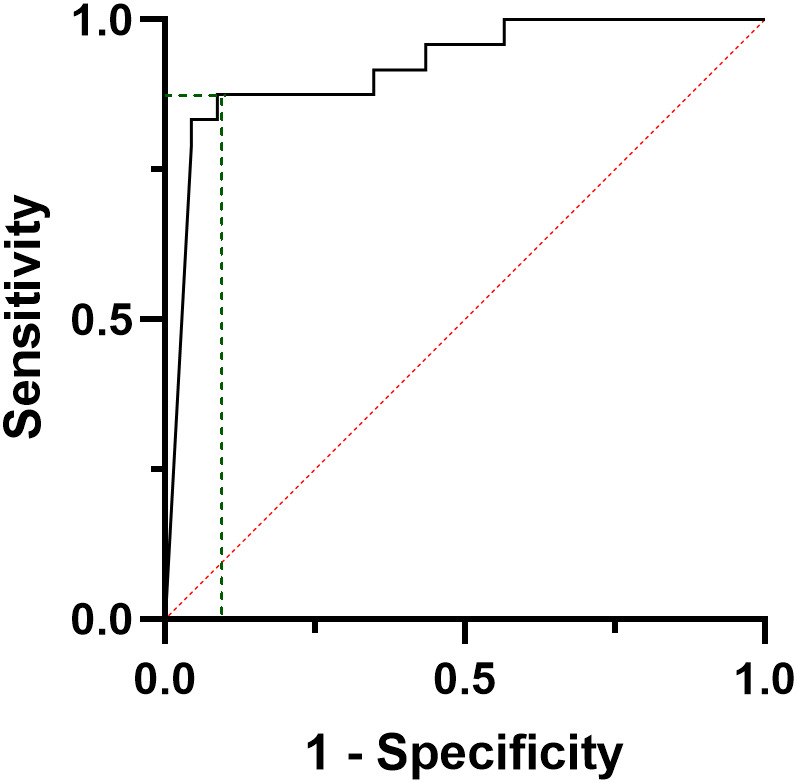
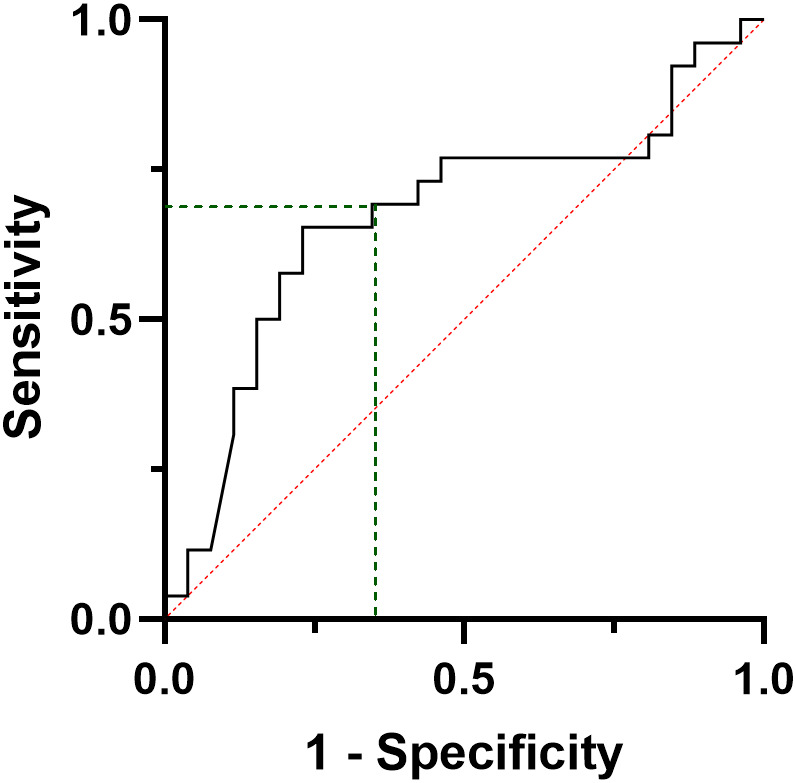
patients showed higher pre-operative and calcitonin values (p=0.028 and p<0.001, respectively), compared to sub-cohort. Cox-regression models show that early detectable calcitonin increases up to 18-fold the risk of persistent disease, independently from tumour size and pre-operative calcitonin levels (p=0.006). Of note, when considering only patients who finally developed distant metastasis, ROC curve analysis shows that an calcitonin level ≥16 pg/ml predicts the final disease status with a sensitivity of 89% and a specificity of 82% (AUC=0.911, CI95%: 0.819-1000, p<0.001).
Calcitonin levels six months after surgery represents an easy and effective predictor of persistent disease for medullary thyroid carcinoma without distant metastasis at diagnosis.
降钙素是甲状腺髓样癌最具特异性的标志物,因此,术后可检测到的降钙素值较低可能掩盖疾病的持续存在。本研究旨在探讨术前和术后降钙素水平在诊断时无远处转移患者中的预后作用。
纳入一组甲状腺髓样癌患者的回顾性队列(N = 55)。根据最后一次可用的随访结果推断最终疾病状态,即(降钙素水平不可检测且影像学评估为阴性)或(降钙素水平可检测且/或影像学评估为阳性)。根据最终疾病状态,将术前和术后降钙素水平(即术后六个月)与若干临床和组织学特征进行关联。
与亚组相比,患者术前和术后降钙素值更高(分别为p = 0.028和p < 0.001)。Cox回归模型显示,早期可检测到的降钙素使疾病持续风险增加至18倍,与肿瘤大小和术前降钙素水平无关(p = 0.006)。值得注意的是,仅考虑最终发生远处转移的患者时,ROC曲线分析显示,术后降钙素水平≥16 pg/ml预测最终疾病状态的敏感性为89%,特异性为82%(AUC = 0.911,CI95%:0.819 - 1000,p < 0.001)。
术后六个月的降钙素水平是诊断时无远处转移的甲状腺髓样癌疾病持续的简便有效预测指标。