Division of Medical Oncology, Mayo Clinic, Rochester, Minnesota, USA.
Department of Oncology, Clínica Santa María, Santiago, Chile.
Prostate. 2023 May;83(7):649-655. doi: 10.1002/pros.24498. Epub 2023 Mar 16.
Elevated serum chromogranin A (CGA) is associated with intrinsic or treatment-related neuroendocrine differentiation (NED) in men with metastatic castration-resistant prostate cancer (mCRPC). Fluctuations in serum CGA during treatment of mCRPC have had conflicting results. We analyzed the impact of (i) rising serum CGA and (ii) baseline CGA/PSA ratio during treatment to identify associations with abiraterone acetate (AA) therapy.
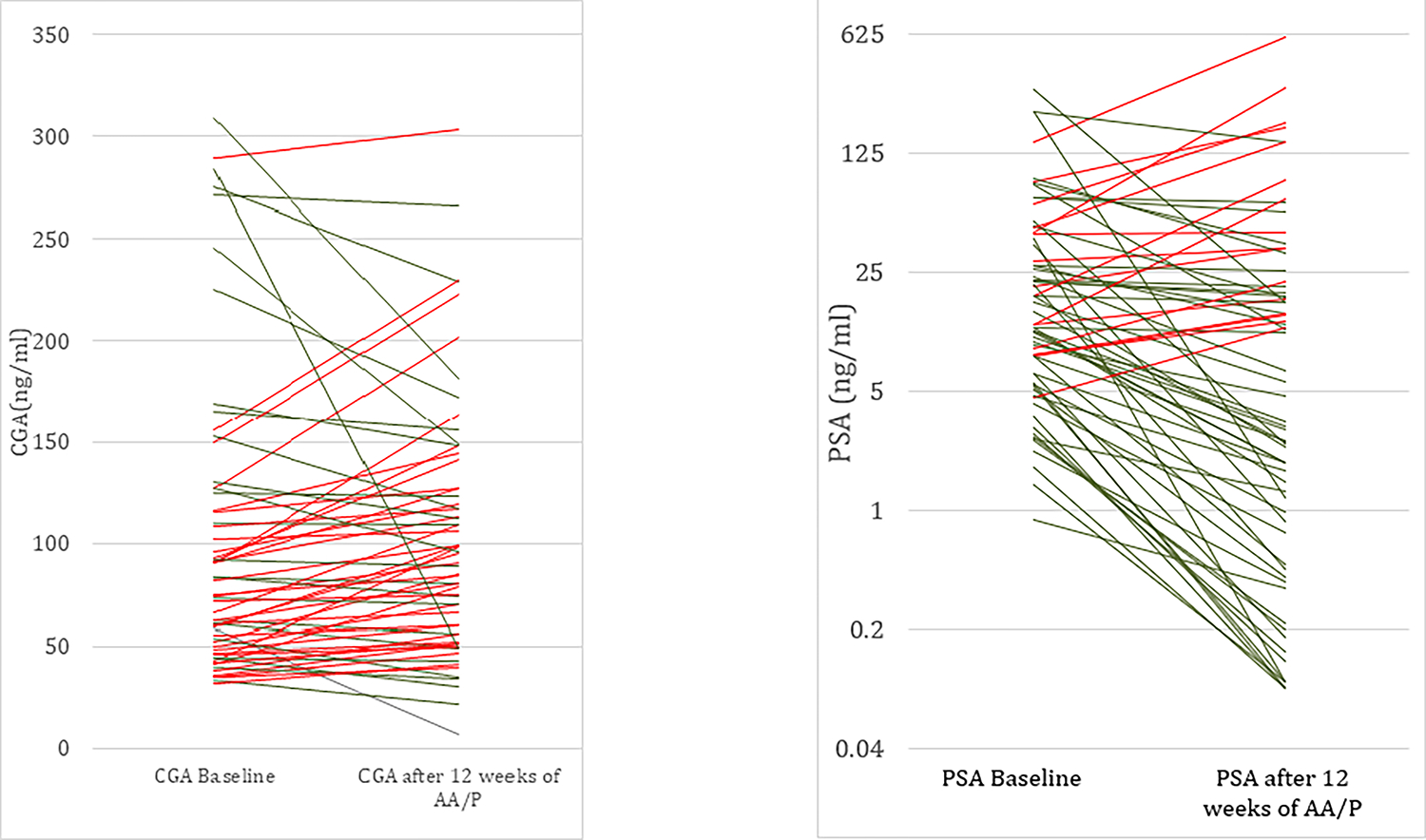
Between June 2013 and August 2015, 92 men with mCRPC were enrolled in a prospective trial with uniform serum CGA processing performed before initiating abiraterone acetate/prednisone (AA/P) and serially after 12 weeks of AA/P treatments. Serum CGA was measured using a homogenous automated immunofluorescent assay. Patients receiving proton pump inhibitors or with abnormal renal function were excluded due to possible false elevations of serum CGA (n = 21 excluded), therefore 71 patients were analyzed. All patients underwent a composite response assessment at 12-weeks. Kaplan-Meier estimates and Cox Regression models were used to calculate the association with time-to-treatment failure analyses and overall survival.
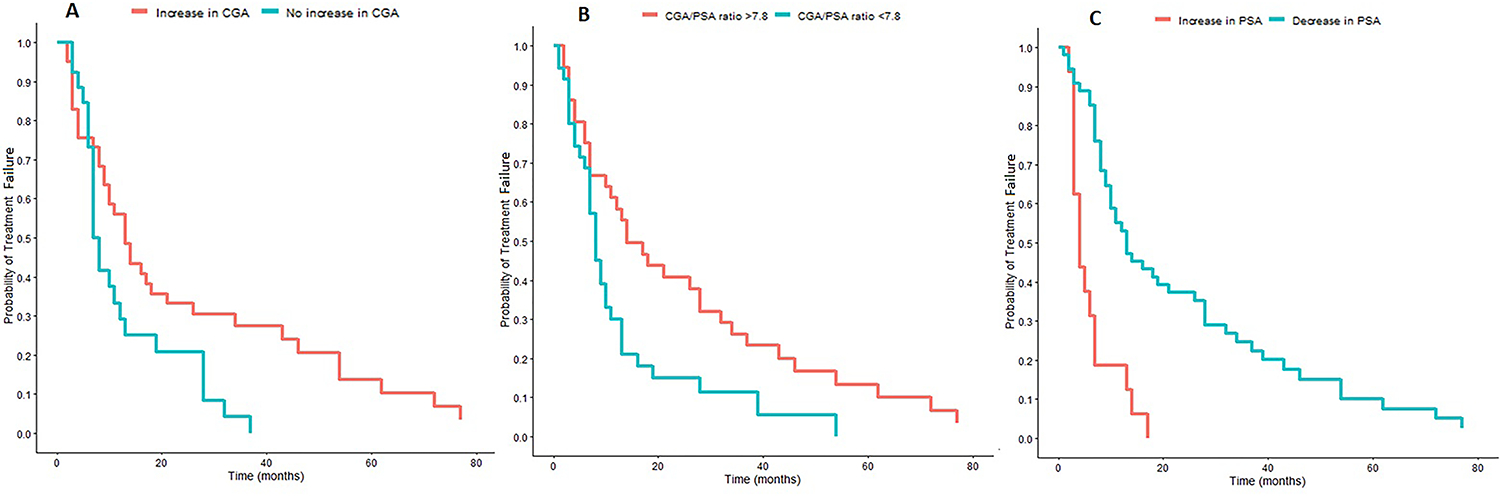
An increase in chromogranin was associated with a lower risk of treatment failure (hazard ratio [HR]: 0.52, p = 0.0181). The median CGA/PSA ratio was 7.8 (2.6-16.0) and an elevated pretreatment CGA/PSA ratio above the median was associated with a lower risk of treatment failure (HR: 0.54 p value = 0.0185). An increase in CGA was not found to be associated with OS (HR: 0.71, 95% CI: 0.42-1.21, p = 0.207). An elevated baseline CGA/PSA ratio was not associated with OS (HR: 0.62, 95% CI: 0.37-1.03, p = 0.062). An increase in PSA after 12 weeks of treatment was associated with an increased risk of treatment failure (HR: 4.14, CI: 2.21-7.73, p = < 0.0001) and worse OS (HR: 2.93, CI: 1.57-4.45, p = < 0.0001).
We show that an increasing chromogranin on AA/P and an elevated baseline CGA/PSA in patients with mCRPC were associated with a favorable response to AA/P with no changes in survival. There may be limited clinical utility in serum CGA testing to evaluate for lethal NED as AA/P did not induce lethal NED in this cohort. This highlights that not all patients with an increasing CGA have a worse OS.
在转移性去势抵抗性前列腺癌(mCRPC)患者中,血清嗜铬粒蛋白 A(CGA)升高与内在或治疗相关的神经内分泌分化(NED)有关。在 mCRPC 的治疗过程中,血清 CGA 的波动结果存在矛盾。我们分析了(i)血清 CGA 升高和(ii)治疗期间基线 CGA/PSA 比值的变化,以确定与醋酸阿比特龙(AA)治疗的关联。
2013 年 6 月至 2015 年 8 月,92 名 mCRPC 患者入组了一项前瞻性试验,在开始使用醋酸阿比特龙/泼尼松(AA/P)前和 AA/P 治疗 12 周后连续进行统一的血清 CGA 处理。使用均相自动荧光免疫测定法测量血清 CGA。由于可能存在血清 CGA 的假升高(排除了 21 例异常患者),因此排除了接受质子泵抑制剂或肾功能异常的患者,因此对 71 名患者进行了分析。所有患者在 12 周时进行了综合反应评估。Kaplan-Meier 估计和 Cox 回归模型用于计算与治疗失败分析和总生存时间的关联。
CGA 升高与治疗失败风险降低相关(风险比 [HR]:0.52,p=0.0181)。CGA/PSA 比值的中位数为 7.8(2.6-16.0),预处理时高于中位数的 CGA/PSA 比值与治疗失败风险降低相关(HR:0.54,p 值=0.0185)。CGA 升高与 OS 无关(HR:0.71,95%CI:0.42-1.21,p=0.207)。基线 CGA/PSA 比值升高与 OS 无关(HR:0.62,95%CI:0.37-1.03,p=0.062)。治疗 12 周后 PSA 升高与治疗失败风险增加相关(HR:4.14,CI:2.21-7.73,p<0.0001)和 OS 恶化相关(HR:2.93,CI:1.57-4.45,p<0.0001)。
我们表明,在接受 AA/P 治疗的 mCRPC 患者中,CGA 增加和基线时 CGA/PSA 升高与 AA/P 治疗的良好反应相关,而生存无变化。在该队列中,AA/P 并未诱导致命性 NED,因此血清 CGA 检测评估致死性 NED 的临床应用可能有限。这突出表明,并非所有 CGA 升高的患者 OS 都较差。