Division of Cardiology, Yunnan Arrhythmia Research Center, the First People's Hospital of Yunnan Province, the Affiliated Hospital of Kunming University of Science and Technology, China (X.K., X.Z., Y.C., F.W., P.W., X.G., H.X., H.W., L.-L.W., J.F.).
CRHF Division, Medtronic PLC, Mounds View, MN (X.Z.).
Circ Arrhythm Electrophysiol. 2023 Apr;16(4):e011408. doi: 10.1161/CIRCEP.122.011408. Epub 2023 Mar 16.
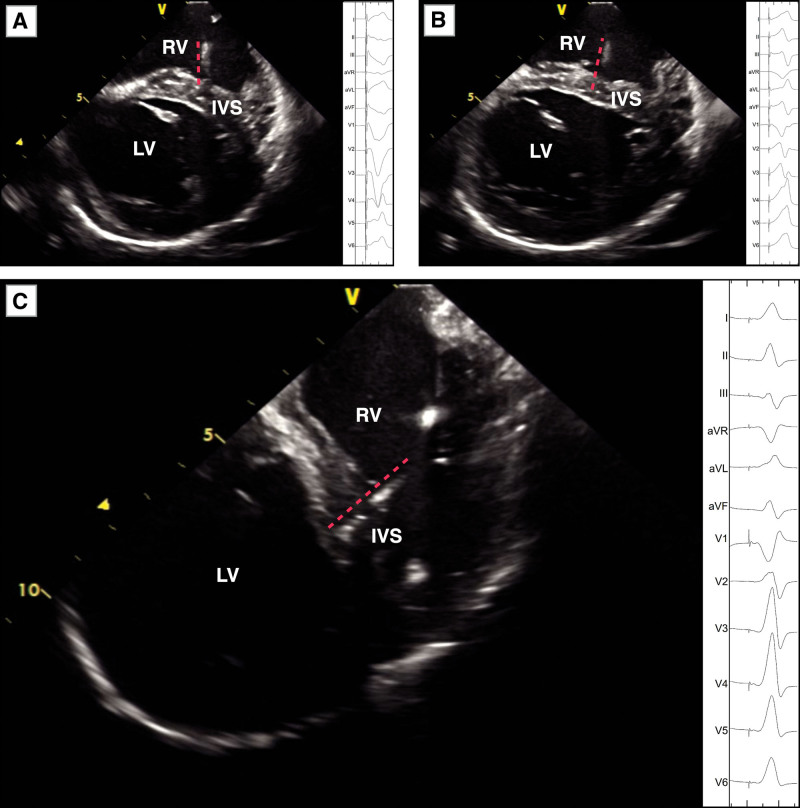
Multiple screw-in attempts under fluoroscopy are often needed to place the pacing lead tip near or at the left bundle branch (LBB). This study was conducted to evaluate the feasibility of implanting an LBB pacing lead in the proximal LBB (PLBB) guided by intracardiac echocardiography (ICE).
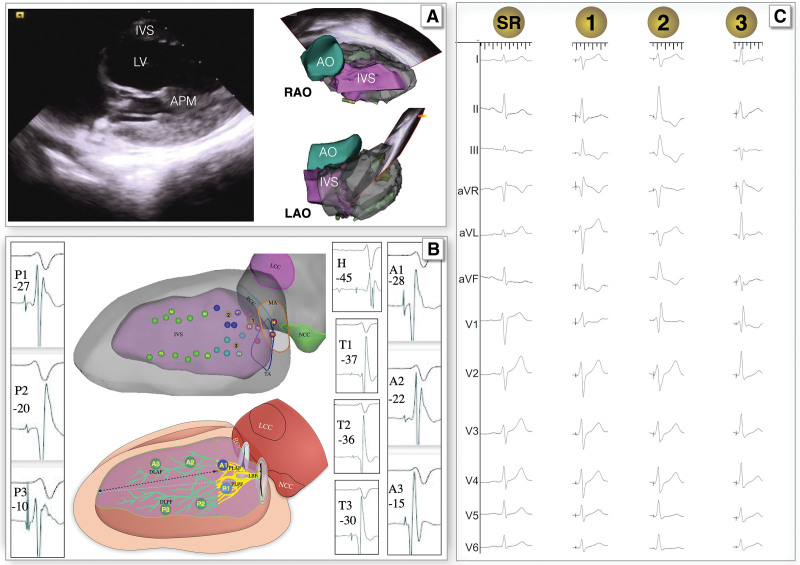
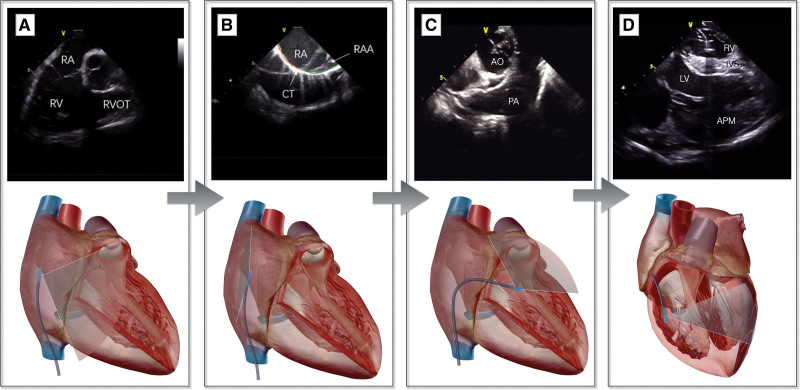
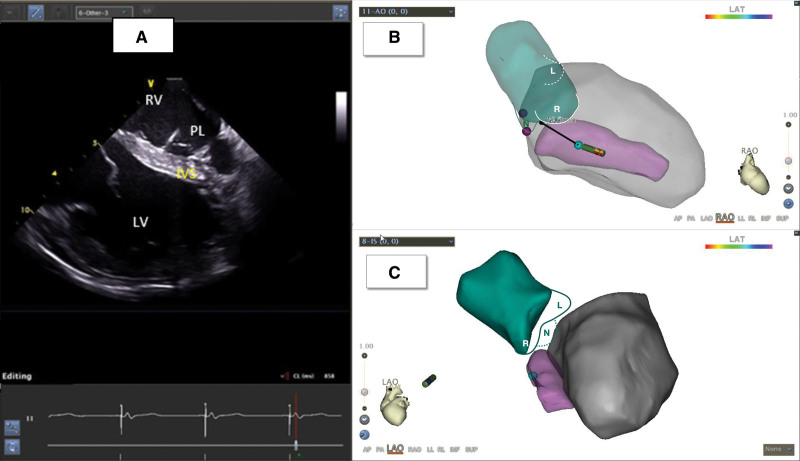
The distribution of the LBB was initially determined by ICE anatomic imaging and 3-dimensional electrical mapping of His and LBB potentials in 20 patients in the first parts of the study. In the second part, 101 consecutive pacemaker-indicated patients were randomized into the ICE-guided and non-ICE groups for LBB pacing implantation. The procedural details and electrophysiological characteristics of the 2 groups were compared.
In the first part of the study, PLBB was identified at 10 to 20 mm from the tricuspid annulus toward the apex with an area of 4.5±1.1 cm. In the second part, the number of lead screw-in attempts in the septum was fewer in the ICE group than in the non-ICE group (1.43±0.62 versus 1.98±0.75, =0.0002). The duration of the procedure (26±8 versus 43±9 minutes, <0.001) and fluoroscopy for LBB pacing implantation (7.4±1.8 versus 10.7±2.4 minutes, <0.001) in the ICE group was significantly shorter than those in the non-ICE group. LBB pacing in the ICE group generated a lesser QRS duration with more cases of LBB trunk pacing (46.8% versus 25%, =0.031) and PLBB (91.5% versus 72.7%, =0.0267) pacing compared with that in the non-ICE group.
The basal left ventricular septum can be better visualized using ICE. ICE-guided PLBB pacing is feasible and safe, with a shorter duration required for the procedure and fluoroscopy, and generates greater LBB trunk pacing and PLBB pacing.
在透视引导下,通常需要多次尝试将起搏导线尖端放置在左束支(LBB)附近或处。本研究旨在评估在心脏内超声心动图(ICE)引导下植入 LBB 起搏导线的可行性。
在研究的第一部分,通过 ICE 解剖成像和希氏束和 LBB 电位的 3 维电描记图初步确定 LBB 的分布。在第二部分,将 101 例连续的起搏器指征患者随机分为 ICE 引导组和非 ICE 组进行 LBB 起搏植入。比较两组的手术细节和电生理特征。
在研究的第一部分,在距离三尖瓣环 10 至 20mm 处向心尖方向的间隔内识别出 PLBB,面积为 4.5±1.1cm。在第二部分,ICE 组比非 ICE 组在间隔内导丝插入次数更少(1.43±0.62 比 1.98±0.75,=0.0002)。ICE 组的手术时间(26±8 比 43±9 分钟,<0.001)和 LBB 起搏植入的透视时间(7.4±1.8 比 10.7±2.4 分钟,<0.001)明显短于非 ICE 组。ICE 组的 LBB 起搏产生的 QRS 持续时间更短,并且 LBB 干起搏(46.8%比 25%,=0.031)和 PLBB(91.5%比 72.7%,=0.0267)起搏的病例更多。
ICE 可更好地显示左心室间隔基底部。ICE 引导的 PLBB 起搏是可行且安全的,需要的手术和透视时间更短,产生更大的 LBB 干起搏和 PLBB 起搏。