Vink Coralien H, Logt Anne-Els van de, van der Molen Renate G, Hofstra Julia M, Wetzels Jack F M
Department of Nephrology, Radboud Institute of Health Sciences, Radboud University Medical Centre, Nijmegen, the Netherlands.
Department of Immunology, Radboud University Medical Centre, Nijmegen, the Netherlands.
Kidney Int Rep. 2022 Dec 13;8(3):432-441. doi: 10.1016/j.ekir.2022.12.003. eCollection 2023 Mar.
A 6-month course of cyclophosphamide (CP) and steroids is effective in primary membranous nephropathy (MN), but unappealing because of long-term side effects. We evaluated efficacy of an "antibody-guided" treatment schedule.
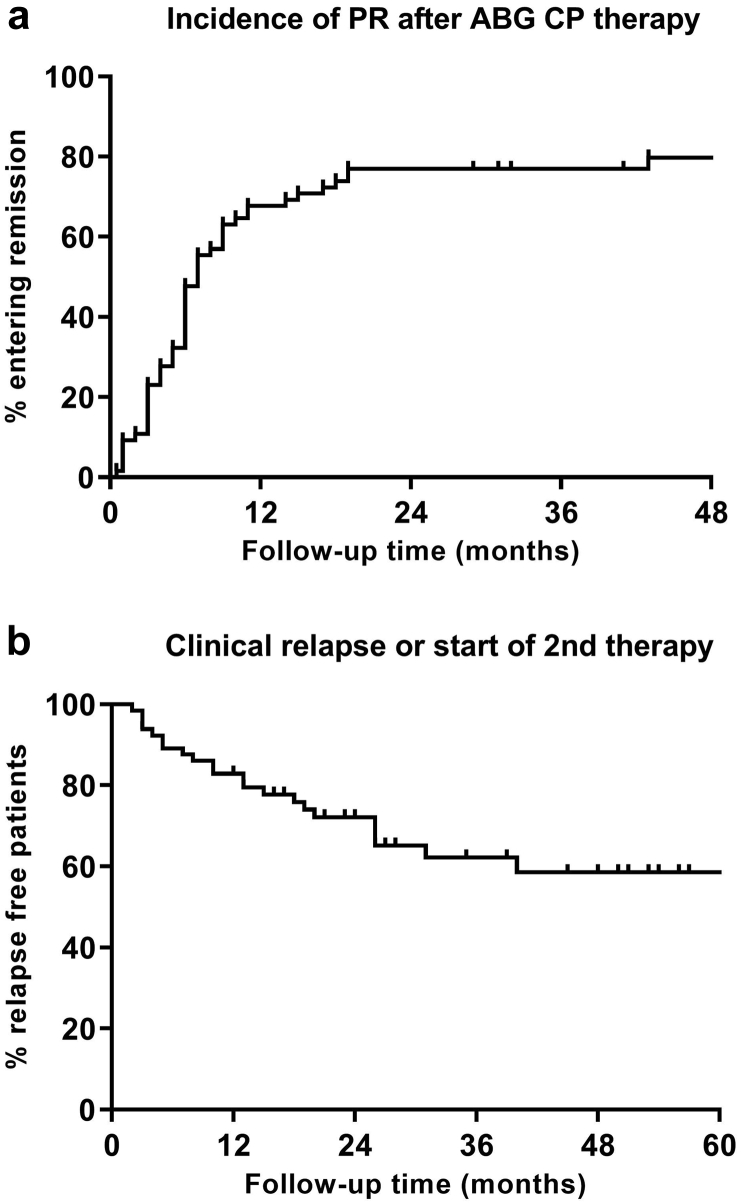
Patients with phospholipase A2 receptor (PLA2R)-related MN and high risk of progression were treated with CP 1.5 mg/kg/d and steroids in cycles of 8 weeks. Anti-PLA2R antibodies were measured by indirect immunofluorescence (IIFT) at 8, 16, and 24 weeks, and a negative test resulted in withdrawal of CP, and rapid tapering of prednisone. In patients with persistent anti-PLA2R antibodies at 24 weeks, CP was switched to mycophenolate mofetil. Treatment was repeated in patients with a relapse.
Our analysis included 65 patients (48 males, 17 females), age 61 ± 12 years, estimated glomerular filtration rate (eGFR) 46 ml/min per 1.73 m (35-68), urine protein-to-creatinine ratio 7.7 grams/10 mmol creatinine (5.4-11.1) and serum albumin 20 g/l (16-26). Immunologic remission rate was 71% after 8 weeks, 86% after 16 weeks, 88% after 24 weeks, and 94% after 3 years. Twenty-seven patients (42%) had persistent clinical remission after only 8 weeks of therapy. Sixteen patients needed a second course of therapy because of immunologic or clinical relapse. Follow-up was 37 (26-58) months. Overall partial remission rate was 92%. One patient developed end-stage kidney disease. Antibody-guided therapy (ABG) was as effective as the standard 6-month course, whereas providing a lower cumulative dose of CP (11.1 [8.0-18.5] vs. 18.9 [14.2-23.6] grams).
ABG is effective, and allows individualized therapy, with many patients responding to 8 weeks of CP-based therapy.
环磷酰胺(CP)和类固醇的6个月疗程对原发性膜性肾病(MN)有效,但因其长期副作用而缺乏吸引力。我们评估了一种“抗体引导”治疗方案的疗效。
患有磷脂酶A2受体(PLA2R)相关MN且进展风险高的患者接受CP 1.5mg/kg/d和类固醇治疗,疗程为8周。在第8、16和24周通过间接免疫荧光法(IIFT)检测抗PLA2R抗体,检测结果为阴性则停用CP,并迅速减量泼尼松。在24周时仍存在抗PLA2R抗体的患者,将CP换为霉酚酸酯。复发患者重复治疗。
我们的分析纳入了65例患者(48例男性,17例女性),年龄61±12岁,估计肾小球滤过率(eGFR)为每1.73平方米46ml/min(35 - 68),尿蛋白与肌酐比值为7.7克/10mmol肌酐(5.4 - 11.1),血清白蛋白20g/l(16 - 26)。8周时免疫缓解率为71%,16周时为86%,24周时为88%,3年后为94%。27例患者(42%)仅经过8周治疗后就实现了持续的临床缓解。16例患者因免疫或临床复发需要第二个疗程的治疗。随访时间为37(26 - 58)个月。总体部分缓解率为92%。1例患者发展为终末期肾病。抗体引导治疗(ABG)与标准的6个月疗程一样有效,同时CP的累积剂量更低(11.1 [8.0 - 18.5]克对18.9 [14.2 - 23.6]克)。
ABG有效,且允许个体化治疗,许多患者对8周的基于CP的治疗有反应。