Farooqui Naba, Zaidi Mark, Vaughan Lisa, McKee Trevor D, Ahsan Eram, Pavelko Kevin D, Villasboas Jose C, Markovic Svetomir, Taner Timucin, Leung Nelson, Dong Haidong, Alexander Mariam P, Herrmann Sandra M
Division of Nephrology and Hypertension, Mayo Clinic, Rochester, Minnesota, USA.
Department of Medical Biophysics, University of Toronto, Ontario, Canada.
Kidney Int Rep. 2022 Dec 5;8(3):628-641. doi: 10.1016/j.ekir.2022.11.020. eCollection 2023 Mar.
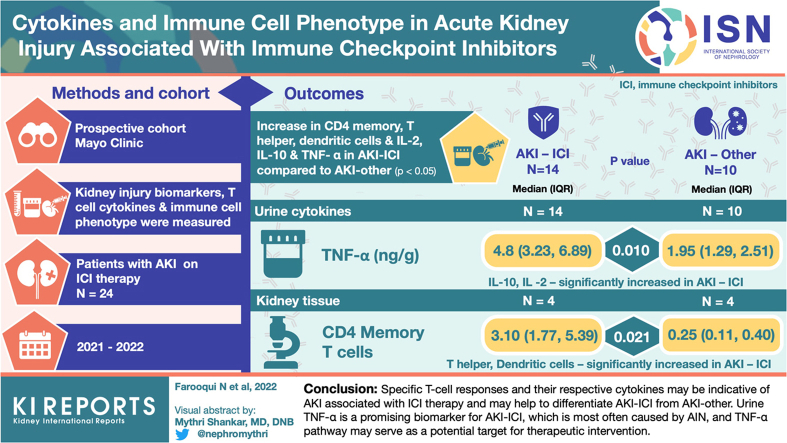
Immune checkpoint inhibitors (ICIs) induce impressive antitumor responses but may lead to acute kidney injury (AKI) associated with ICI therapy (AKI-ICI). Biomarkers distinguishing AKI-ICI from AKI because of other causes (AKI-other) are currently lacking. Because ICIs block immunoregulatory pathways, we hypothesized that biomarkers related to immune cell dysregulation, including tumor necrosis factor alpha (TNF-α) and other markers of B and T cell activation in the systemic circulation and kidney tissue, may aid with the diagnosis of AKI-ICI.
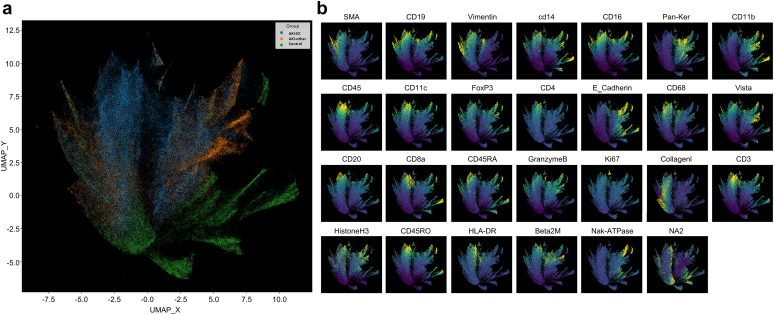
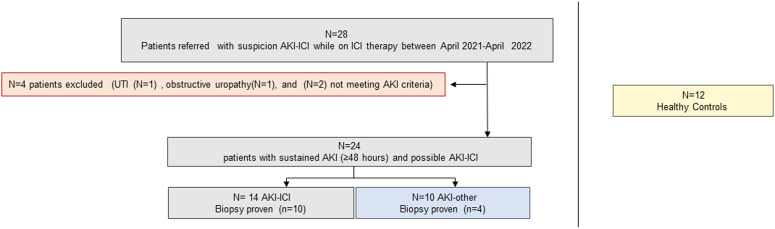
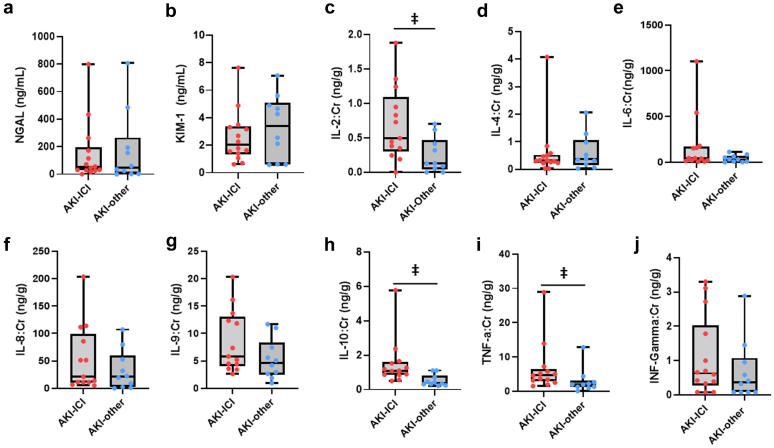
This is a prospective study consisting of 24 participants who presented with AKI during ICI therapy, adjudicated to either have AKI-ICI ( = 14) or AKI-other ( = 10). We compared markers of kidney inflammation and injury (neutrophil gelatinase-associated lipocalin, kidney injury molecule-1) as well as plasma and urine levels of T cell-associated cytokines (TNF-α, interferon-γ, interleukin (IL)-2, IL-4, IL-6, IL-8, IL-9, and IL-10) between groups. We also compared T-cell responses in the systemic circulation and in kidney tissue across groups, using mass cytometry systems.
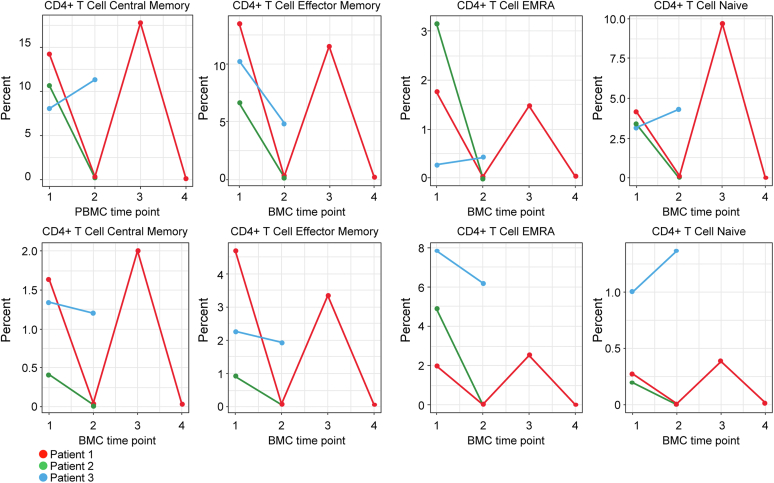
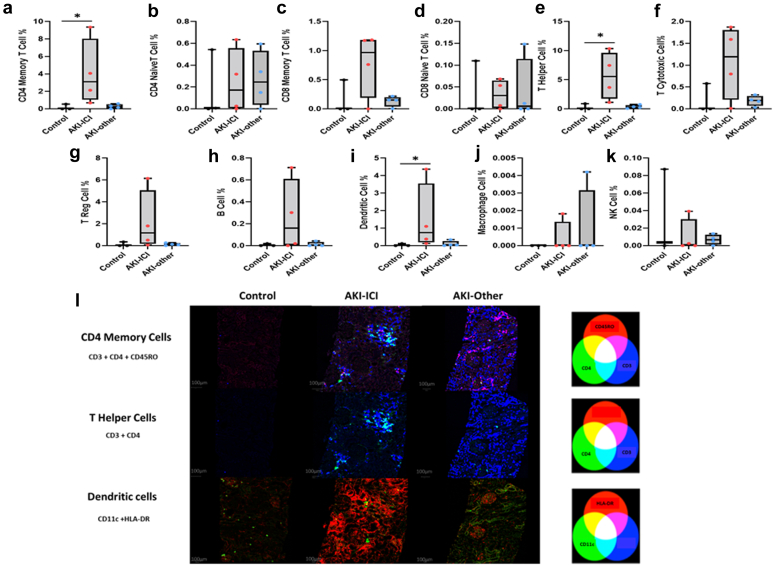
We observed increase in several specific immune cells, including CD4 memory, T helper cells, and dendritic cells in the kidney tissue, as well as in the urine cytokines IL-2, IL-10, and TNF-α, in patients who developed AKI-ICI compared to patients with AKI-other ( < 0.05 for all). The discriminatory ability of TNF-α on AKI cause was strong (area under the curve = 0.814, 95% confidence interval: 0.623-1.00. The CD4+ T cells with memory phenotype formed the dominant subset.
These results suggest that specific T-cell responses and their respective cytokines may be indicative of AKI associated with ICI therapy and may help to differentiate AKI-ICI from AKI-other. Urine TNF-α is a promising biomarker for AKI-ICI, which is most often caused by acute interstitial nephritis (AIN), and TNF-α pathway may serve as a potential target for therapeutic intervention.
免疫检查点抑制剂(ICI)可引发显著的抗肿瘤反应,但可能导致与ICI治疗相关的急性肾损伤(AKI-ICI)。目前缺乏能够区分AKI-ICI与其他原因所致急性肾损伤(AKI-其他原因)的生物标志物。由于ICI阻断免疫调节通路,我们推测与免疫细胞失调相关的生物标志物,包括全身循环和肾组织中的肿瘤坏死因子α(TNF-α)以及B和T细胞活化的其他标志物,可能有助于AKI-ICI的诊断。
这是一项前瞻性研究,纳入了24例在ICI治疗期间出现急性肾损伤的参与者,经判定分为AKI-ICI组(n = 14)和AKI-其他原因组(n = 10)。我们比较了两组间肾炎症和损伤标志物(中性粒细胞明胶酶相关脂质运载蛋白、肾损伤分子-1)以及T细胞相关细胞因子(TNF-α、干扰素-γ、白细胞介素(IL)-2、IL-4、IL-6、IL-8、IL-9和IL-10)的血浆和尿液水平。我们还使用质谱流式细胞术系统比较了两组全身循环和肾组织中的T细胞反应。
与AKI-其他原因组患者相比,发生AKI-ICI的患者肾组织中包括CD4记忆性T辅助细胞和树突状细胞在内的几种特定免疫细胞增加,尿液细胞因子IL-2、IL-10和TNF-α也增加(所有P < 0.05)。TNF-α对AKI病因的鉴别能力较强(曲线下面积 = 0.814,95%置信区间:0.623 - 1.00)。具有记忆表型的CD4 + T细胞构成主要亚群。
这些结果表明,特定的T细胞反应及其各自的细胞因子可能提示与ICI治疗相关的急性肾损伤,并可能有助于区分AKI-ICI与AKI-其他原因。尿液TNF-α是AKI-ICI很有前景的生物标志物,AKI-ICI最常见的病因是急性间质性肾炎(AIN),TNF-α通路可能成为治疗干预的潜在靶点。