Gately Ryan, Milanzi Elasma, Lim Wai, Teixeira-Pinto Armando, Clayton Phil, Isbel Nicole, Johnson David W, Hawley Carmel, Campbell Scott, Wong Germaine
Department of Nephrology, Princess Alexandra Hospital, Queensland, Australia.
Australasian Kidney Trials Network, University of Queensland, Brisbane, Australia.
Kidney Int Rep. 2022 Dec 30;8(3):531-543. doi: 10.1016/j.ekir.2022.12.020. eCollection 2023 Mar.
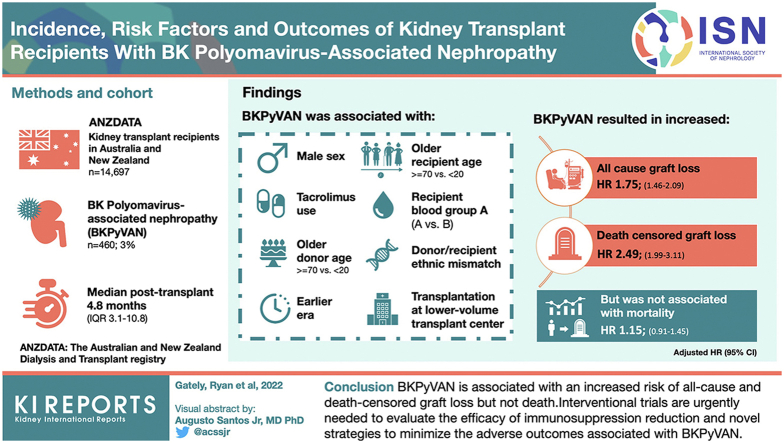
BK polyomavirus-associated nephropathy (BKPyVAN) is associated with graft dysfunction and loss; however, knowledge of immunosuppression reduction strategies and long-term graft, and patient outcomes across the disease spectrum is lacking.
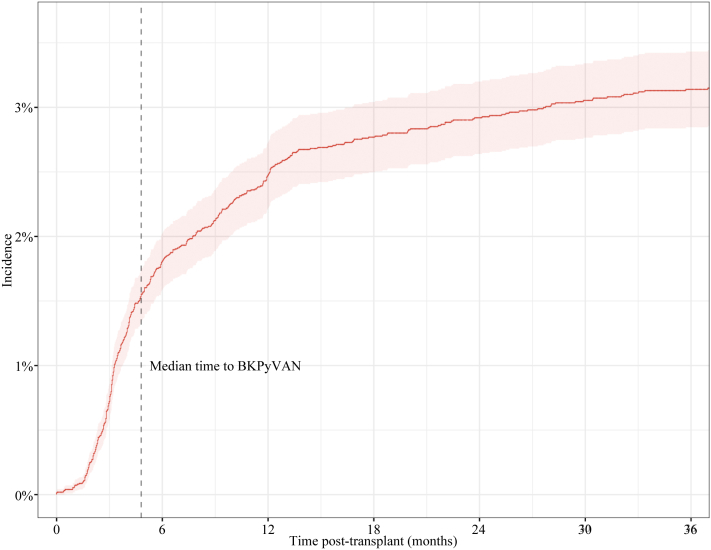
This cohort study included 14,697 kidney transplant recipients in Australia and New Zealand (2005-2019), followed for 91,306 person years.
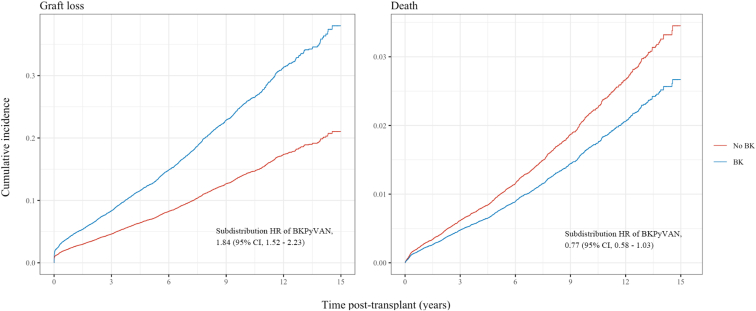
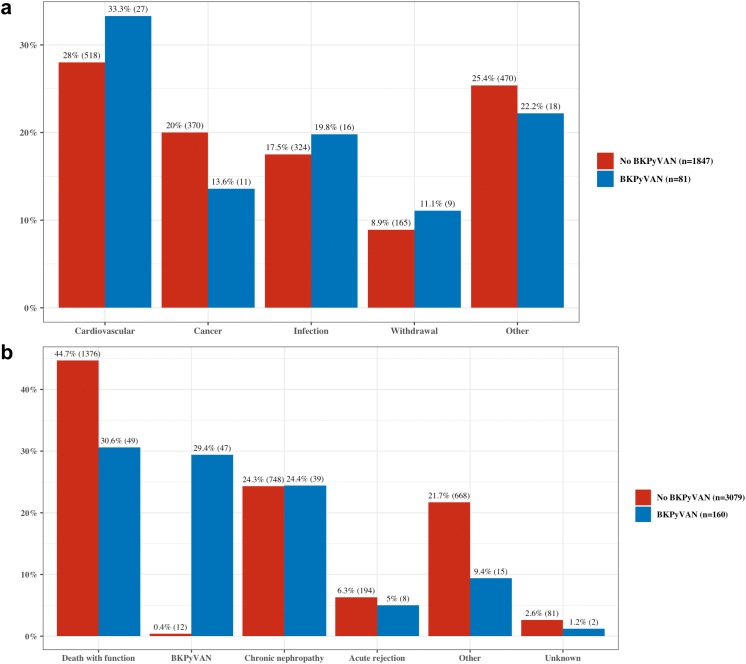
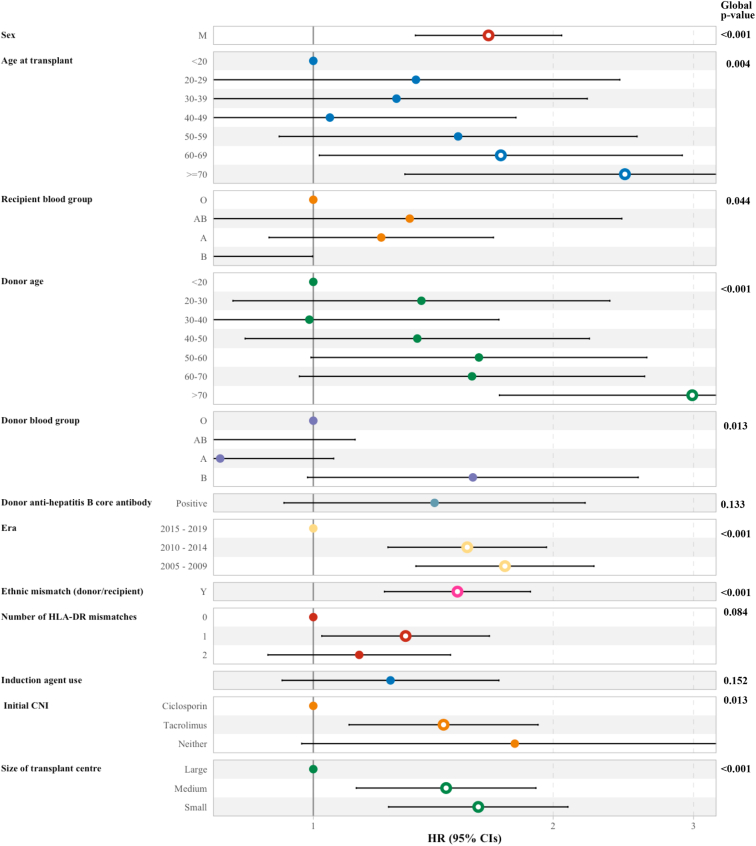
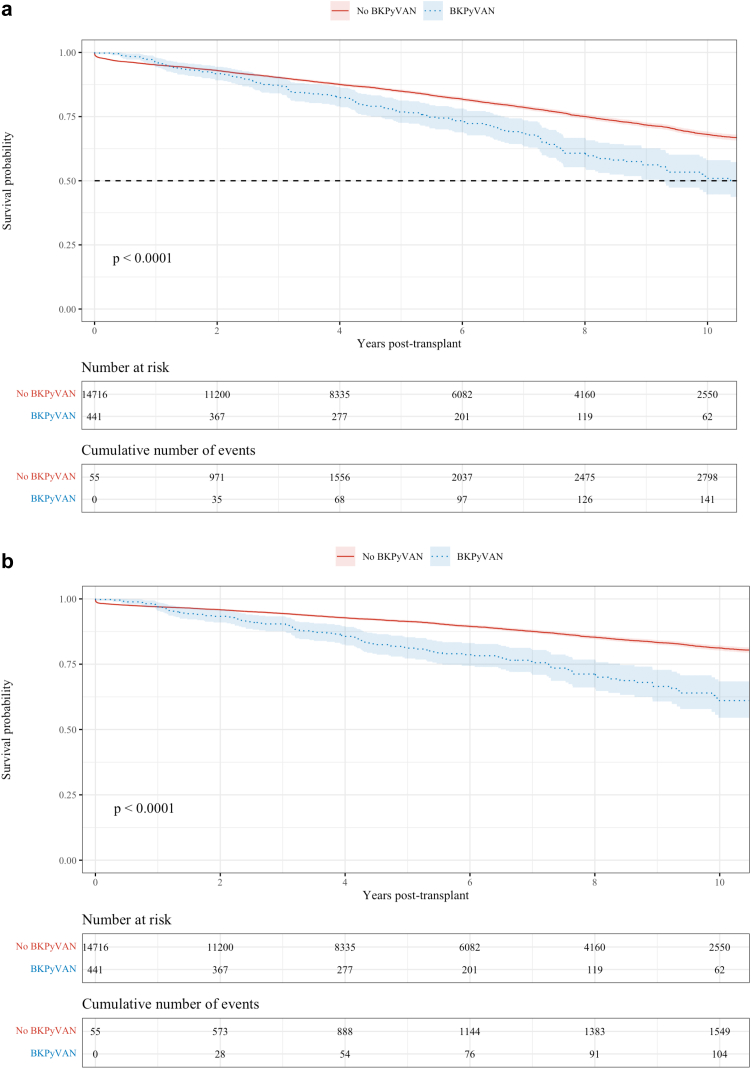
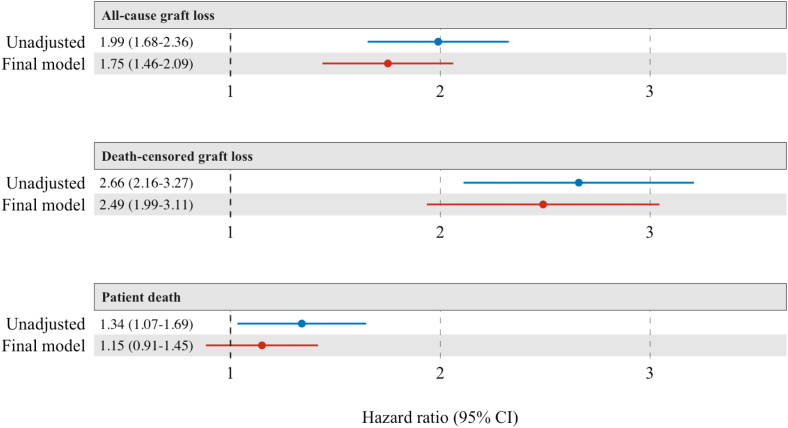
BKPyVAN occurred in 460 recipients (3%) at a median posttransplant time of 4.8 months (interquartile range, 3.1-10.8). Graft loss (35% vs. 21%, < 0.001), rejection (42% vs. 25%, < 0.001), and death (18% vs. 13%, = 0.002) were more common in the BKPyVAN group. The most frequent changes in immunosuppression after BKPyVAN were reduction (≤50%) in tacrolimus (172, 51%) and mycophenolate doses (134, 40%), followed by the conversion of mycophenolate to leflunomide (62, 19%) and tacrolimus to ciclosporin (20, 6%). Factors associated with the development of BKPyVAN included (adjusted hazard ratio [HR]; 95% confidence interval) male sex (1.66; 1.34-2.05), recipient age (≥70 vs. <20 [2.46; 1.30-4.65]), recipient blood group (A vs. B [2.00; 1.19-3.34]), donor age (≥70 vs. <20 [2.99; 1.71-5.22]), earlier era (1.74; 1.35-2.25), donor/recipient ethnic mismatch (1.52; 1.23-1.87), tacrolimus use (1.46; 1.11-1.91), and transplantation at a lower-volume transplant center (1.61; 1.24-2.09). The development of BKPyVAN was associated with an increased risk of all-cause (1.75; 1.46-2.09) and death-censored graft loss (2.49; 1.99-3.11), but not mortality (1.15; 0.91-1.45).
BKPyVAN is associated with an increased risk of all-cause and death-censored graft loss, but not death. Interventional trials are urgently needed to evaluate the efficacy of immunosuppression reduction and novel strategies to minimize the adverse outcomes associated with BKPyVAN.
BK多瘤病毒相关性肾病(BKPyVAN)与移植肾功能障碍及丧失有关;然而,目前缺乏关于免疫抑制减量策略以及疾病全谱中移植肾长期情况和患者预后的相关知识。
这项队列研究纳入了澳大利亚和新西兰的14697名肾移植受者(2005 - 2019年),随访时间达91306人年。
460名受者(3%)发生了BKPyVAN,移植后中位时间为4.8个月(四分位间距为3.1 - 10.8个月)。BKPyVAN组移植肾丧失(35%对21%,<0.001)、排斥反应(42%对25%,<0.001)和死亡(18%对13%,=0.002)更为常见。BKPyVAN发生后免疫抑制最常见的变化是他克莫司剂量减少(≤50%)(172例,51%)和霉酚酸酯剂量减少(134例,40%),其次是霉酚酸酯转换为来氟米特(62例,19%)以及他克莫司转换为环孢素(20例,6%)。与BKPyVAN发生相关的因素包括(校正风险比[HR];95%置信区间)男性(1.66;1.34 - 2.05)、受者年龄(≥70岁对<20岁[2.46;1.30 - 4.65])、受者血型(A型对B型[2.00;1.19 - 3.34])、供者年龄(≥70岁对<20岁[2.99;1.71 - 5.22])、较早时期(1.74;1.35 - 2.25)、供者/受者种族不匹配(1.52;1.23 - 1.87)、使用他克莫司(1.46;1.11 - 1.91)以及在移植量较低的移植中心进行移植(1.61;1.24 - 2.09)。BKPyVAN的发生与全因风险增加(1.75;1.46 - 2.09)和死亡删失的移植肾丧失风险增加(2.49;1.99 - 3.11)相关,但与死亡率无关(1.15;0.91 - 1.45)。
BKPyVAN与全因风险及死亡删失的移植肾丧失风险增加相关,但与死亡无关。迫切需要进行干预性试验以评估免疫抑制减量的疗效以及新策略,以尽量减少与BKPyVAN相关的不良后果。