Division of Nephrology and Hypertension, Mayo Clinic, Rochester, Minnesota.
Division of Clinical Trials and Biostatistics, Mayo Clinic, Rochester, Minnesota.
J Am Soc Nephrol. 2023 Jul 1;34(7):1264-1278. doi: 10.1681/ASN.0000000000000124. Epub 2023 Mar 23.
Nephron number currently can be estimated only from glomerular density on a kidney biopsy combined with cortical volume from kidney imaging. Because of measurement biases, refinement of this approach and validation across different patient populations have been needed. The prognostic importance of nephron number also has been unclear. The authors present an improved method of estimating nephron number that corrects for several biases, resulting in a 27% higher nephron number estimate for donor kidneys compared with a prior method. After accounting for comorbidities, the new nephron number estimate does not differ between kidney donors and kidney patients with tumor and shows consistent associations with clinical characteristics across these two populations. The findings also indicate that low nephron number predicts CKD independent of biopsy and clinical characteristics in both populations.
Nephron number can be estimated from glomerular density and cortical volume. However, because of measurement biases, this approach needs refinement, comparison between disparate populations, and evaluation as a predictor of CKD outcomes.
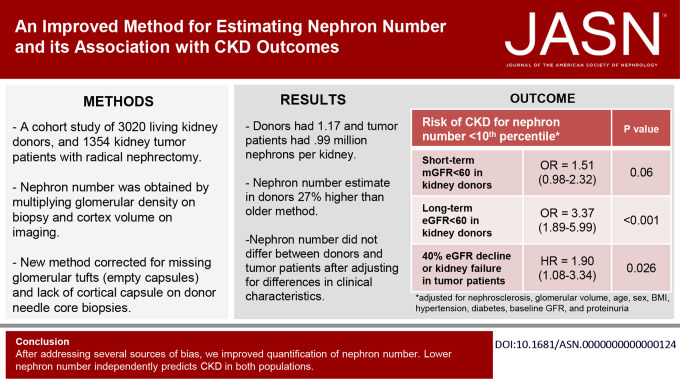
We studied 3020 living kidney donors and 1354 patients who underwent radical nephrectomy for tumor. We determined cortex volume of the retained kidney from presurgical imaging and glomerular density by morphometric analysis of needle core biopsy of the donated kidney and wedge sections of the removed kidney. Glomerular density was corrected for missing glomerular tufts, absence of the kidney capsule, and then tissue shrinkage on the basis of analysis of 30 autopsy kidneys. We used logistic regression (in donors) and Cox proportional hazard models (in patients with tumor) to assess the risk of CKD outcomes associated with nephron number.
Donors had 1.17 million nephrons per kidney; patients with tumor had 0.99 million nephrons per kidney. A lower nephron number was associated with older age, female sex, shorter height, hypertension, family history of ESKD, lower GFR, and proteinuria. After adjusting for these characteristics, nephron number did not differ between donors and patients with tumor. Low nephron number (defined by <5th or <10th percentile by age and sex in a healthy subset) in both populations predicted future risk of CKD outcomes independent of biopsy and clinical characteristics.
Compared with an older method for estimating nephron number, a new method that addresses several sources of bias results in nephron number estimates that are 27% higher in donors and 1% higher in patients with tumor and shows consistency between two populations. Low nephron number independently predicts CKD in both populations.
目前,肾小球密度与肾脏成像的皮质体积结合起来,可以估算出肾小球数量。但是,由于测量偏差,需要对该方法进行改进,并在不同的患者群体中进行验证。肾小球数量的预后意义也不明确。作者提出了一种改进的肾小球数量估计方法,可以纠正几种偏差,与以前的方法相比,供体肾脏的肾小球数量估计值提高了 27%。在考虑合并症后,新的肾小球数量估计值在供体肾脏和患有肿瘤的肾脏患者之间没有差异,并在这两个人群中表现出与临床特征一致的关联。研究结果还表明,低肾小球数量独立于活检和临床特征预测 CKD,在这两个人群中都是如此。
肾小球数量可以通过肾小球密度和皮质体积来估计。但是,由于测量偏差,需要对该方法进行改进,在不同的人群中进行比较,并将其作为 CKD 结果的预测因子进行评估。
我们研究了 3020 名活体供肾者和 1354 名因肿瘤接受根治性肾切除术的患者。我们通过对供肾的针芯活检和切除肾的楔形切片进行形态计量学分析,确定保留肾的皮质体积,并通过肾小球密度确定肾小球密度。在基于 30 例尸检肾脏的分析的基础上,对缺失的肾小球簇、无肾脏包膜以及随后的组织收缩进行校正。我们使用逻辑回归(供体中)和 Cox 比例风险模型(肿瘤患者中)来评估与肾小球数量相关的 CKD 结果的风险。
供体的每只肾脏有 117 万个肾小球;肿瘤患者的每只肾脏有 99 万个肾小球。肾小球数量较少与年龄较大、女性、身高较矮、高血压、ESKD 家族史、较低的肾小球滤过率和蛋白尿有关。在调整这些特征后,供体与肿瘤患者的肾小球数量没有差异。在两个群体中,肾小球数量较少(在健康亚组中按年龄和性别定义为 <第 5 或 <第 10 百分位数)与未来 CKD 结果的风险独立于活检和临床特征相关。
与以前的肾小球数量估计方法相比,一种新的方法可以纠正几个来源的偏差,结果是供体的肾小球数量估计值提高了 27%,肿瘤患者的肾小球数量估计值提高了 1%,并且在两个群体之间具有一致性。低肾小球数量独立于活检和临床特征预测 CKD,在两个群体中都是如此。