Endocrine Surgery Unit, Royal North Shore Hospital, Northern Sydney Local Health District, St Leonards, NSW 2065, Australia.
The Kinghorn Cancer Centre, Garvan Institute of Medical Research, St Vincent's Clinical School, Faculty of Medicine, University of New South Wales, Darlinghurst, NSW 2010, Australia.
J Clin Endocrinol Metab. 2023 Sep 18;108(10):2626-2634. doi: 10.1210/clinem/dgad173.
Management of sporadic medullary thyroid microcarcinoma smaller than 1 cm (micro-MTC) is controversial because of conflicting reports of prognosis. As these cancers are often diagnosed incidentally, they pose a management challenge when deciding on further treatment and follow-up.
We report the outcomes of surgically managed sporadic micro-MTC in a specialist endocrine surgery and endocrinology unit and identify associations for recurrence and disease-specific survival in this population.
Micro-MTCs were identified from a prospectively maintained surgery database, and slides were reviewed to determine pathological grade. The primary end points were recurrence, time to recurrence and disease-specific survival. Prognostic factors assessed included size, grade, lymph node metastasis (LNM), and postoperative calcitonin.
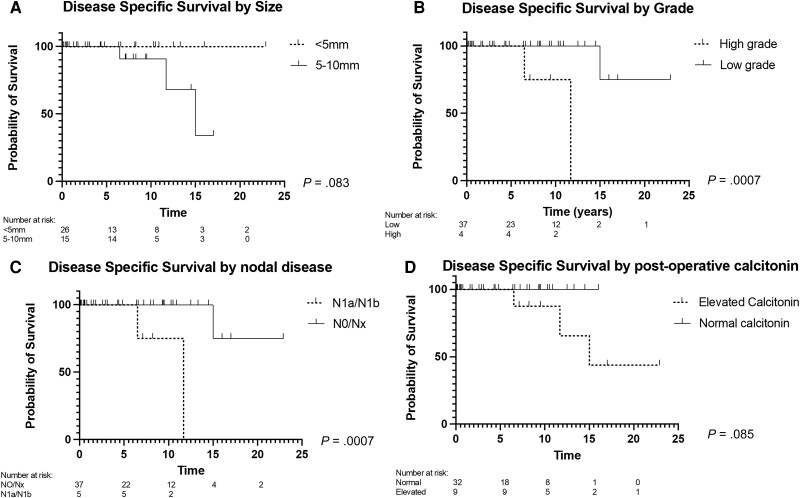
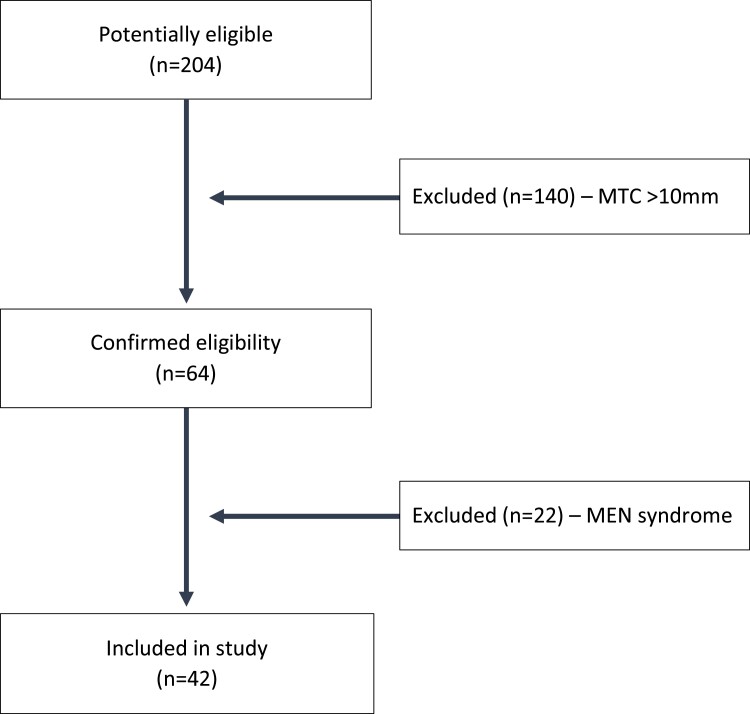
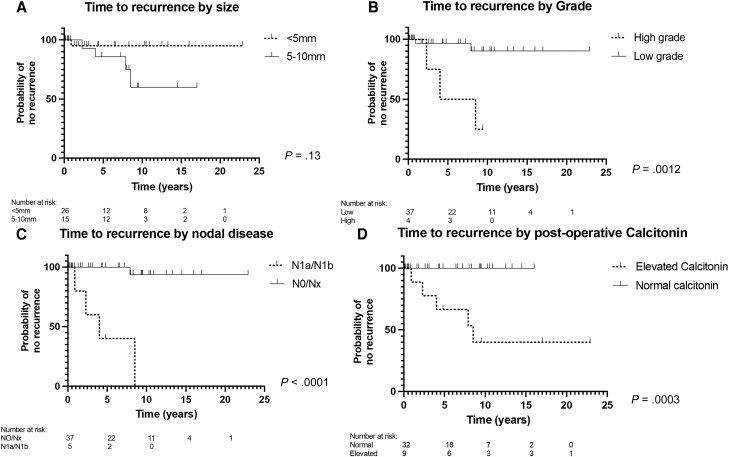
From 1995 to 2022, 64 patients were diagnosed with micro-MTC with 22 excluded because of hereditary disease. The included patients had a median age of 60 years, tumor size of 4 mm, and 28 (67%) were female. The diagnosis was incidental in 36 (86%) with 4 (10%) being high grade, 5 (12%) having LNM and 9 (21%) having elevated postoperative calcitonin. Over a 6.6-year median follow-up, 5 (12%) developed recurrence and 3 (7%) died of MTC. High grade and LNM were associated with 10-year survival estimates of 75% vs 100% for low grade and no LNM (hazard ratio = 831; P < .01). High grade, LNM, and increased calcitonin were associated with recurrence (P < .01). Tumor size and type of surgery were not statistically significantly associated with recurrence or survival. No patients with low grade micro-MTC and normal postoperative calcitonin developed recurrence.
Most sporadic micro-MTCs are detected incidentally and are generally associated with good outcomes. Size is not significantly associated with outcomes. Using grade, LNM, and postoperative calcitonin allows for the identification of patients at risk of recurrence to personalize management.
1cm 以下散发性甲状腺髓样癌(微癌)的管理存在争议,因为预后的报告相互矛盾。由于这些癌症通常是偶然诊断出来的,因此在决定进一步治疗和随访时,这给管理带来了挑战。
我们报告了在一个内分泌外科和内分泌学专科单位中,对手术治疗的散发性微髓样癌的结果,并确定了该人群中复发和疾病特异性生存的相关因素。
从一个前瞻性维持的手术数据库中确定微髓样癌病例,并对切片进行审查以确定病理分级。主要终点是复发、复发时间和疾病特异性生存。评估的预后因素包括大小、分级、淋巴结转移(LNM)和术后降钙素。
1995 年至 2022 年,64 例患者被诊断为微髓样癌,其中 22 例因遗传性疾病被排除在外。纳入的患者中位年龄为 60 岁,肿瘤大小为 4mm,28 例(67%)为女性。36 例(86%)为偶然诊断,其中 4 例(10%)为高级别,5 例(12%)有 LNM,9 例(21%)术后降钙素升高。在中位随访 6.6 年后,5 例(12%)发生复发,3 例(7%)死于髓样癌。高级别和 LNM 与低级别和无 LNM 的 10 年生存率估计值分别为 75%和 100%(风险比=831;P<.01)相关。高级别、LNM 和升高的降钙素与复发相关(P<.01)。肿瘤大小和手术类型与复发或生存无统计学显著相关性。无低级别微髓样癌和术后降钙素正常的患者发生复发。
大多数散发性微髓样癌是偶然发现的,通常预后良好。大小与结局无显著相关性。使用分级、LNM 和术后降钙素可识别有复发风险的患者,从而实现个体化管理。