Swami Vivekananda Yoga Anusandhana Samsthana, Bengaluru, India.
Narayana Health City, Bengaluru, India.
Front Public Health. 2023 Mar 9;11:1054207. doi: 10.3389/fpubh.2023.1054207. eCollection 2023.
The initial insights from the studies on COVID-19 had been disappointing, indicating the necessity of an aggravated search for alternative strategies. In this regard, the adjunct potential of yoga has been proposed for enhancing the effectiveness of the standard of care with respect to COVID-19 management. We tested whether a telemodel of yoga intervention could aid in better clinical management for hospitalized patients with mild-to-moderate COVID-19 when complemented with the standard of care.
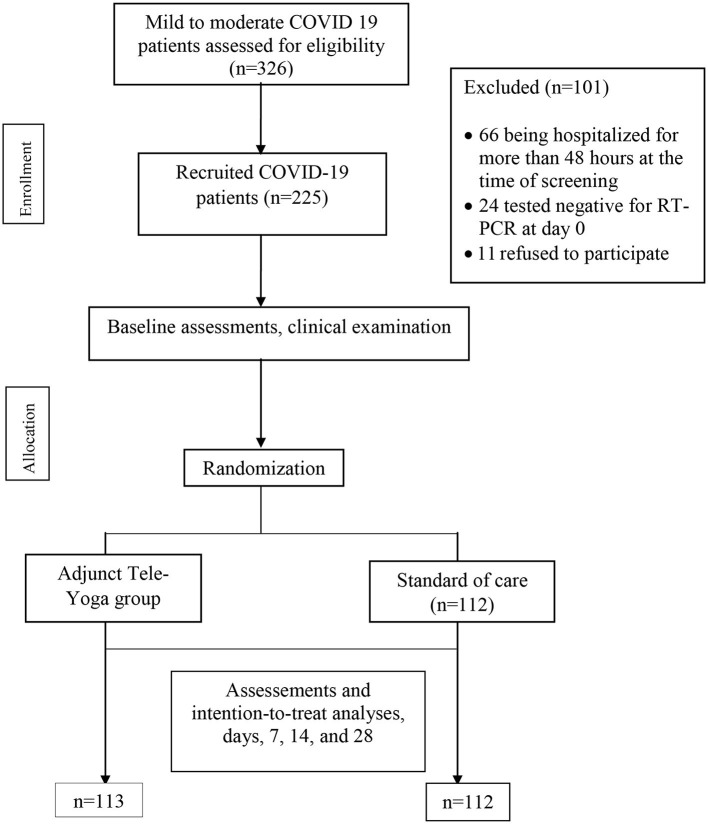
This was a randomized controlled trial conducted at the Narayana Hrudyalaya, Bengaluru, India, on hospitalized patients with mild-to-moderate COVID-19 infection enrolled between 31 May and 22 July 2021. The patients ( = 225) were randomized in a 1:1 ratio [adjunct tele-yoga ( = 113) or standard of care]. The adjunct yoga group received intervention in tele-mode within 4-h post-randomization until 14 days along with the standard of care. The primary outcome was the clinical status on day 14 post-randomization, assessed with a seven-category ordinal scale. The secondary outcome set included scores on the COVID Outcomes Scale on day 7, follow-up for clinical status and all-cause mortality on day 28, post-randomization, duration of days at the hospital, 5th-day changes post-randomization for viral load expressed as cyclic threshold (Ct), and inflammatory markers and perceived stress scores on day 14.
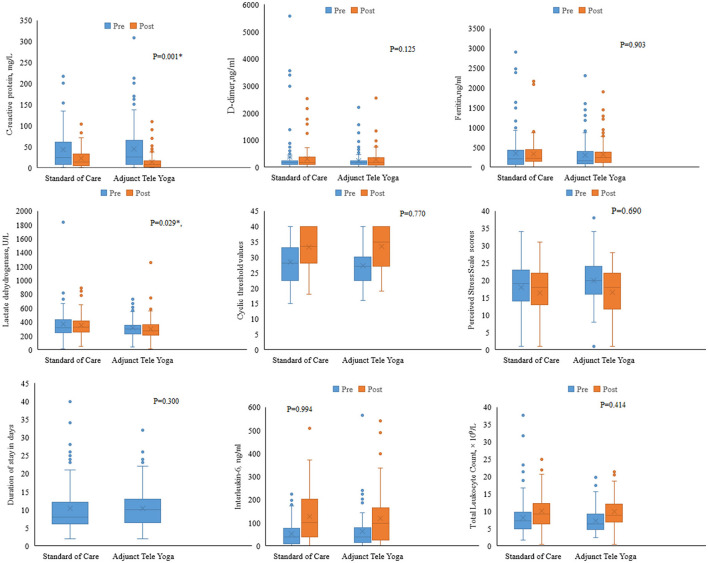
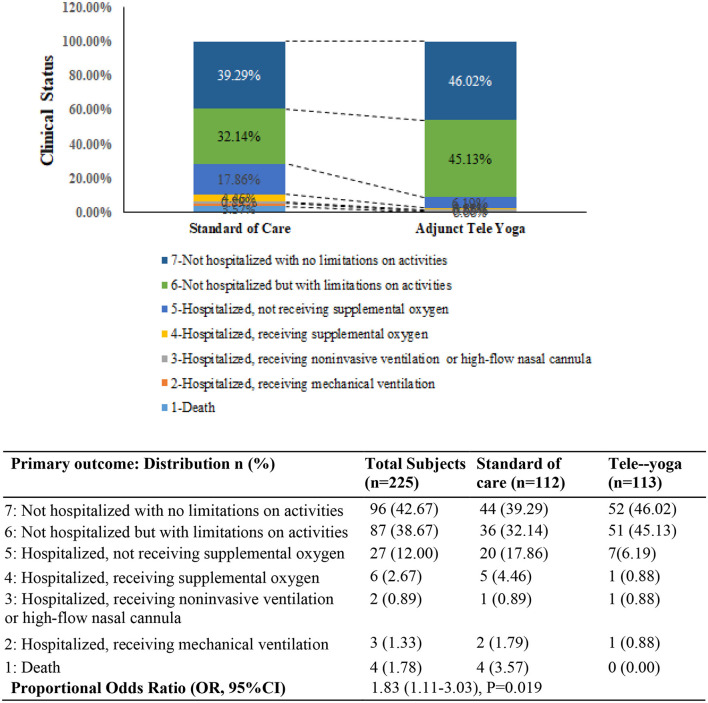
As compared with the standard of care alone, the proportional odds of having a higher score on the 7-point ordinal scale on day 14 were ~1.8 for the adjunct tele-yoga group (OR = 1.83, 95% CI, 1.11-3.03). On day 5, there were significant reductions in CRP ( = 0.001) and LDH levels ( = 0.029) in the adjunct yoga group compared to the standard of care alone. CRP reduction was also observed as a potential mediator for the yoga-induced improvement of clinical outcomes. The Kaplan-Meier estimate of all-cause mortality on day 28 was the adjusted hazard ratio (HR) of 0.26 (95% CI, 0.05-1.30).
The observed 1.8-fold improvement in the clinical status on day 14 of patients of COVID-19 with adjunct use of tele-yoga contests its use as a complementary treatment in hospital settings.
最初对 COVID-19 的研究结果令人失望,表明有必要寻找更具创新性的策略。在这方面,瑜伽的辅助作用已经被提出,以提高标准治疗方法对 COVID-19 管理的有效性。我们测试了在补充标准治疗的情况下,远程瑜伽干预模式是否可以帮助改善轻度至中度 COVID-19 住院患者的临床管理。
这是一项在印度班加罗尔的 Narayana Hrudyalaya 进行的随机对照试验,于 2021 年 5 月 31 日至 7 月 22 日期间纳入患有轻度至中度 COVID-19 感染的住院患者。患者(n=225)按照 1:1 的比例随机分配[辅助远程瑜伽(n=113)或标准治疗]。辅助瑜伽组在随机分组后 4 小时内以远程模式接受干预,持续 14 天,同时接受标准治疗。主要结局是随机分组后第 14 天的临床状态,采用 7 级有序量表评估。次要结局包括第 7 天 COVID 结局量表评分、第 28 天随访的临床状态和全因死亡率、随机分组后第 28 天的住院天数、随机分组后第 5 天病毒载量的循环阈值(Ct)变化、第 14 天的炎症标志物和感知压力评分。
与单独接受标准治疗相比,第 14 天采用 7 点有序量表评分较高的比例,辅助远程瑜伽组约为 1.8(OR=1.83,95%CI,1.11-3.03)。第 5 天,与单独接受标准治疗相比,辅助瑜伽组的 CRP(=0.001)和 LDH 水平(=0.029)显著降低。在瑜伽诱导的临床结局改善方面,CRP 降低也被认为是一种潜在的中介因素。第 28 天全因死亡率的 Kaplan-Meier 估计值为调整后的危险比(HR)为 0.26(95%CI,0.05-1.30)。
辅助远程瑜伽使用的 COVID-19 患者第 14 天临床状态改善 1.8 倍,这表明其在医院环境中作为辅助治疗方法的使用是合理的。