Salem Mohamed, Boehme Maximilian, Friedrich Christine, Ernst Markus, Puehler Thomas, Lutter Georg, Schoeneich Felix, Haneya Assad, Cremer Jochen, Schoettler Jan
Department of Cardiovascular Surgery, University Hospital Schleswig-Holstein, Campus Kiel, 24105 Kiel, Germany.
Department of Pediatric Cardiac Surgery, Pediatric Cardiac Centre, University Hospital of Gießen and Marburg, Campus Gießen, 35385 Gießen, Germany.
J Cardiovasc Dev Dis. 2023 Mar 2;10(3):107. doi: 10.3390/jcdd10030107.
Outcomes after surgical aortic root replacement using different valved conduits are rarely reported. The present study shows the experience of a single center with the use of the partially biological LABCOR (LC) conduit and the fully biological BioIntegral (BI) conduit. Special attention was paid to preoperative endocarditis.
All 266 patients who underwent aortic root replacement by an LC conduit ( = 193) or a BI conduit ( = 73) between 01/01/2014 and 31/12/2020 were studied retrospectively. Dependency on an extracorporeal life support system preoperatively and congenital heart disease were exclusion criteria. For patients with ( = 67) and without ( = 199) preoperative endocarditis subanalyses were made.
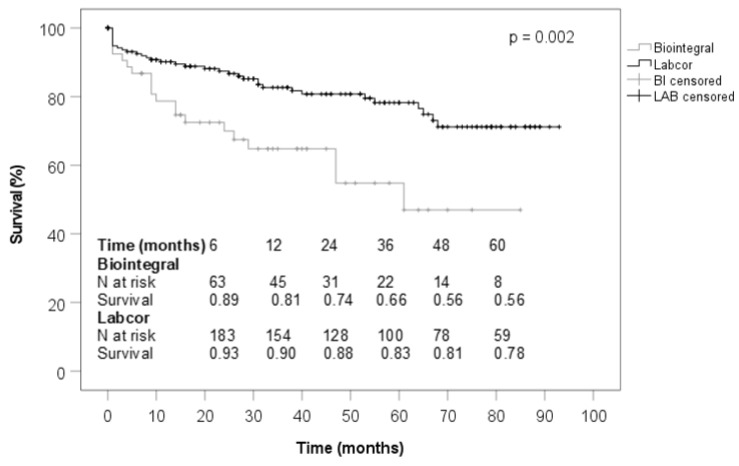
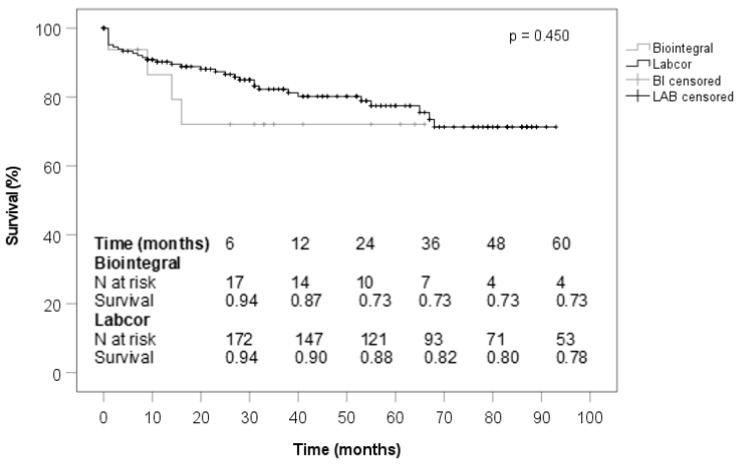
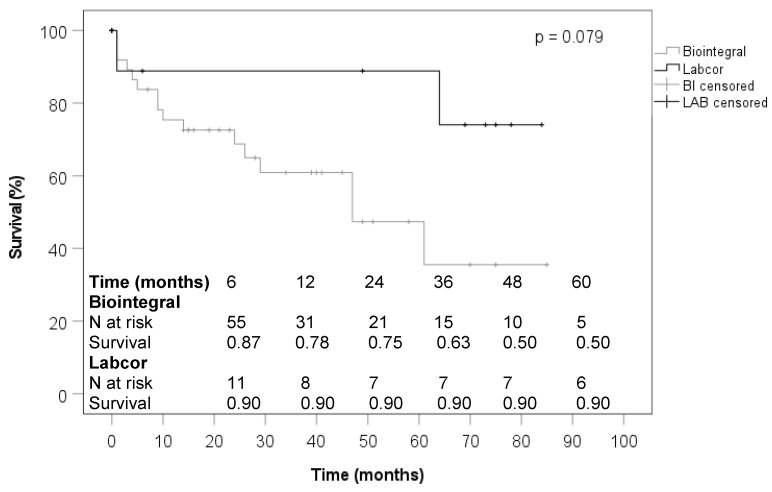
Patients treated with a BI conduit were more likely to have diabetes mellitus (21.9 vs. 6.7%, < 0.001), previous cardiac surgery (86.3 vs. 16.6%; < 0.001), permanent pacemaker (21.9 vs. 2.1%; < 0.001), and had a higher EuroSCORE II (14.9 vs. 4.1%; < 0.001). The BI conduit was used more frequently for prosthetic endocarditis (75.3 vs. 3.6%; <0.001), and the LC conduit was used predominantly for ascending aortic aneurysms (80.3 vs. 41.1%; <0.001) and Stanford type A aortic dissections (24.9 vs. 9.6%; = 0.006). The LC conduit was used more often for elective (61.7 vs. 47.9%; = 0.043) and emergency (27.5 vs. 15.1%; = 0-035) surgeries, and the BI conduit for urgent surgeries (37.0 vs. 10.9%; < 0.001). Conduit sizes did not differ significantly, with a median of 25 mm in each case. Surgical times were longer in the BI group. In the LC group, coronary artery bypass grafting and proximal or total replacement of the aortic arch were combined more frequently, whereas in the BI group, partial replacement of the aortic arch were combined. In the BI group, ICU length of stay and duration of ventilation were longer, and rates of tracheostomy and atrioventricular block, pacemaker dependence, dialysis, and 30-day mortality were higher. Atrial fibrillation occurred more frequently in the LC group. Follow-up time was longer and rates of stroke and cardiac death were less frequent in the LC group. Postoperative echocardiographic findings at follow-up were not significantly different between conduits. Survival of LC patients was better than that of BI patients. In the subanalysis of patients with preoperative endocarditis, significant differences between the used conduits were found with respect to previous cardiac surgery, EuroSCORE II, aortic valve and prosthesis endocarditis, elective operation, duration of operation, and proximal aortic arch replacement. For patients without preoperative endocarditis, significant differences were observed concerning previous cardiac surgery, pacemaker implantation history, duration of procedure, and bypass time. The Kaplan-Meier curves for the subanalyses showed no significant differences between the used conduits.
Both biological conduits studied here are equally suitable in principle for complete replacement of the aortic root in all aortic root pathologies. The BI conduit is often used in bail-out situations, especially in severe endocarditis, without being able to show a clinical advantage over the LC conduit in this context.
使用不同带瓣管道进行主动脉根部置换术后的结果鲜有报道。本研究展示了单中心使用部分生物性LABCOR(LC)管道和全生物性BioIntegral(BI)管道的经验。特别关注了术前心内膜炎情况。
回顾性研究了2014年1月1日至2020年12月31日期间接受LC管道(n = 193)或BI管道(n = 73)主动脉根部置换的所有266例患者。术前依赖体外生命支持系统和先天性心脏病为排除标准。对有(n = 67)和无(n = 199)术前心内膜炎的患者进行了亚组分析。
接受BI管道治疗的患者更易患糖尿病(21.9%对6.7%,P < 0.001)、既往有心脏手术史(86.3%对16.6%;P < 0.001)、植入永久性起搏器(21.9%对2.1%;P < 0.001),且欧洲心脏手术风险评估系统II(EuroSCORE II)更高(14.9%对4.1%;P < 0.001)。BI管道更常用于人工瓣膜心内膜炎(75.3%对3.6%;P<0.001),而LC管道主要用于升主动脉瘤(80.3%对41.1%;P < 0.001)和斯坦福A型主动脉夹层(24.9%对9.6%;P = 0.006)。LC管道更多用于择期手术(61.7%对47.9%;P = 0.043)和急诊手术(27.5%对15.1%;P = 0.035),BI管道用于紧急手术(37.0%对10.9%;P < 0.001)更多。管道尺寸无显著差异,每组中位数均为25mm。BI组手术时间更长。在LC组,冠状动脉旁路移植术与主动脉弓近端或全置换联合应用更频繁,而在BI组,主动脉弓部分置换联合应用更多。在BI组,重症监护病房住院时间和通气时间更长,气管切开率、房室传导阻滞率、起搏器依赖率、透析率和30天死亡率更高。房颤在LC组更常见。LC组随访时间更长,中风和心源性死亡率更低。随访时术后超声心动图检查结果在两种管道间无显著差异。LC组患者生存率优于BI组。在术前有心内膜炎患者的亚组分析中,所用管道在既往心脏手术、EuroSCORE II、主动脉瓣和人工瓣膜心内膜炎、择期手术、手术时间和主动脉弓近端置换方面存在显著差异。对于无术前心内膜炎的患者,在既往心脏手术、起搏器植入史、手术时间和体外循环时间方面观察到显著差异。亚组分析的Kaplan-Meier曲线显示所用管道间无显著差异。
这里研究的两种生物管道原则上同样适用于所有主动脉根部病变的主动脉根部完全置换。BI管道常用于紧急情况,尤其是严重心内膜炎,但在此情况下与LC管道相比未显示出临床优势。