Cummings Mackenzie, Edmonds Pamela, Shahin Mark S, Sorosky Joel I
Jefferson Abington Hospital, Department of Obstetrics and Gynecology, United States.
Jefferson Abington Hospital, Department of Pathology, United States.
Gynecol Oncol Rep. 2023 Mar 17;46:101164. doi: 10.1016/j.gore.2023.101164. eCollection 2023 Apr.
To report a case of stage IIIB juvenile granulosa cell tumor (JGCT) complicating pregnancy in a 33 year-old (y.o.) woman.
Retrospective review of the clinical data, imaging studies, and pathology reports of a case of JGCT diagnosed during pregnancy. Patient consent was obtained for review and presentation of the case. A literature review was conducted.
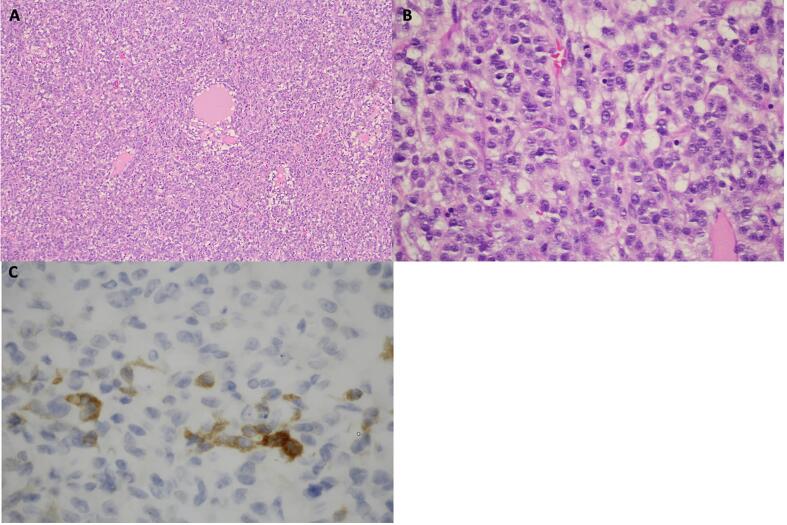
A 33 y.o., gravida 3, para 1 was incidentally found to have an 8 cm left ovarian mass on an anatomy scan at 22 weeks gestation. Four days later, she presented to labor and delivery triage with abdominal pain. An ultrasound revealed an 11 cm heterogeneous, solid mass in the left adnexa and free fluid at this level. The diagnosis of degenerating fibroid was made based on her clinical presentation and she was discharged. A follow up outpatient MRI revealed a 15 cm left ovarian mass consistent with a primary malignant ovarian neoplasm with moderate ascites and omental, left cul de sac, and probable paracolic gutter implantation. She re-presented 2 weeks later with an acute abdomen and was admitted for a gynecologic oncology consult. Pre-op tumor markers showed an elevated inhibin B. She underwent an exploratory laparotomy, left salpingo-oophorectomy, omental biopsy, and small bowel resection at 25 weeks gestation. Intra-op findings included a ruptured tumor and metastases. Tumor reductive surgery was completed to R0. Pathology revealed a JGCT, FIGO stage IIIB. The pathology and management were reviewed in collaboration with an outside institution. Chemotherapy was delayed until after delivery with monthly MRI surveillance. She underwent induction of labor at 37 weeks followed by an uncomplicated vaginal delivery. She received 3 cycles of bleomycin, etoposide, and cisplatin starting six weeks postpartum. Last known contact was over five years after the initial diagnosis with no evidence of recurrent disease.
JGCTs account for 5% of granulosa cell tumors and 3% are diagnosed after age 30. JGCT is an uncommon neoplasm in pregnancy. 90% are stage I at diagnosis, but advanced stage tumors are aggressive often resulting in recurrence or death within 3 years of diagnosis. We present a surgically treated case with delay in chemotherapy until after delivery with a good outcome after 5 years of follow up.
报告一例33岁女性妊娠合并IIIB期青少年颗粒细胞瘤(JGCT)的病例。
回顾性分析一例孕期诊断为JGCT的临床资料、影像学检查及病理报告。已获得患者同意对该病例进行回顾和展示,并进行了文献综述。
一名33岁、孕3产1的女性在妊娠22周时进行解剖扫描时偶然发现左侧卵巢有一个8厘米的肿块。四天后,她因腹痛前往分娩分诊处。超声检查显示左侧附件有一个11厘米的异质性实性肿块,并伴有该水平的游离液体。根据临床表现诊断为变性肌瘤,随后她出院了。门诊后续的MRI检查显示左侧卵巢有一个15厘米的肿块,符合原发性恶性卵巢肿瘤,伴有中度腹水以及网膜、左侧直肠陷凹和可能的结肠旁沟种植转移。两周后她因急腹症再次就诊,并被收入院接受妇科肿瘤会诊。术前肿瘤标志物显示抑制素B升高。她在妊娠25周时接受了剖腹探查术、左侧输卵管卵巢切除术、网膜活检和小肠切除术。术中发现包括肿瘤破裂和转移。肿瘤减瘤手术达到R0切除。病理显示为JGCT,国际妇产科联盟(FIGO)分期为IIIB期。与外部机构合作对病理和治疗进行了复查。化疗推迟至分娩后进行,每月进行MRI监测。她在37周时引产,随后顺利经阴道分娩。产后六周开始接受3个周期的博来霉素、依托泊苷和顺铂化疗。最后一次已知联系是在初次诊断五年多后,没有复发疾病的证据。
JGCT占颗粒细胞瘤的5%,3%在30岁以后被诊断出来。JGCT在妊娠中是一种罕见的肿瘤。90%在诊断时为I期,但晚期肿瘤具有侵袭性,常在诊断后3年内导致复发或死亡。我们报告了一例经手术治疗的病例,化疗推迟至分娩后,随访5年效果良好。