Department of Diagnostics and Public Health, University of Verona, Policlinico G.B. Rossi, P.Le L.A. Scuro, 10, 37138, Verona, Italy.
Department of Biomedical and Dental Sciences and Morpho-Functional Imaging, Unit of Neurosurgery, Messina, Italy.
Virchows Arch. 2023 Jul;483(1):97-104. doi: 10.1007/s00428-023-03537-2. Epub 2023 Apr 4.
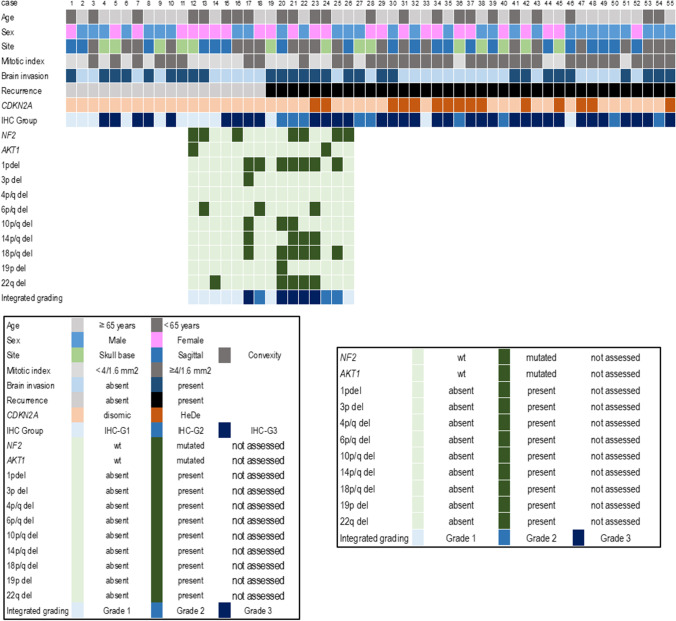
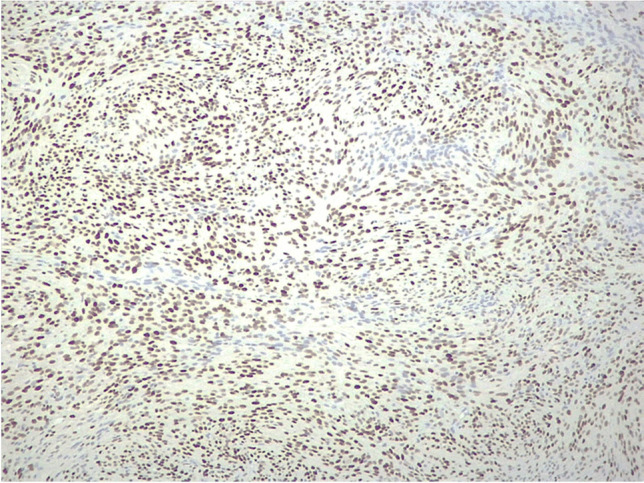
The use of adjuvant radiotherapy is controversial for atypical meningiomas undergoing gross total resection. It has recently been proposed that meningiomas may be classified into four molecular groups (MG): immunogenic (MG1), benign NF2-wildtype (MG2), hypermetabolic (MG3), and proliferative (MG4). The two latter have the worst prognosis, and it has been suggested that they can be identified using ACADL and MCM2 immunostainings. We studied 55 primary atypical meningiomas, treated with gross total resection and no adjuvant therapies, to assess whether ACADL and MCM2 immuno-expression may identify patients at higher recurrence risk, thus requiring adjuvant treatments. Twelve cases resulted ACADL-/MCM2-, 9 ACADL + /MCM2-, 17 ACADL + /MCM2 + , and 17 ACADL-/MCM2 + . MCM2 + meningiomas displayed more frequent atypical features (prominent nucleoli, small cells with high nuclear-to-cytoplasmic ratio) and CDKN2A hemizygous deletion (HeDe) (P = 0.011). The immunoexpression of ACADL and/or MCM2 was significantly associated with higher mitotic index, 1p and 18q deletions, increased recurrence rate (P = 0.0006), and shorter recurrence-free survival (RFS) (P = 0.032). At multivariate analysis, carried out including ACADL/MCM2 immuno-expression, mitotic index, and CDKN2A HeDe as covariates, this latter resulted a significant and independent prognosticator of shorter RFS (P = 0.0003).
辅助放疗在接受大体全切除的非典型脑膜瘤中的应用存在争议。最近有人提出,脑膜瘤可以分为四个分子组(MG):免疫原性(MG1)、良性 NF2 野生型(MG2)、代谢活跃(MG3)和增殖性(MG4)。后两者预后最差,有人建议可以通过 ACADL 和 MCM2 免疫染色来识别。我们研究了 55 例接受大体全切除且未接受辅助治疗的原发性非典型脑膜瘤,以评估 ACADL 和 MCM2 免疫表达是否可以识别具有更高复发风险的患者,从而需要辅助治疗。12 例为 ACADL-/MCM2-,9 例为 ACADL+/MCM2-,17 例为 ACADL+/MCM2+,17 例为 ACADL-/MCM2+。MCM2+脑膜瘤具有更多的非典型特征(明显核仁、小细胞、高核浆比)和 CDKN2A 杂合性缺失(HeDe)(P=0.011)。ACADL 和/或 MCM2 的免疫表达与更高的有丝分裂指数、1p 和 18q 缺失、更高的复发率(P=0.0006)和更短的无复发生存(RFS)(P=0.032)显著相关。在多变量分析中,包括 ACADL/MCM2 免疫表达、有丝分裂指数和 CDKN2A HeDe 作为协变量,后者是 RFS 较短的显著独立预后因素(P=0.0003)。