Wu Shuyi, Guan Chengfu, Xu Wenlin, Zhang Feilong, Huang Nianxu, Chen Xia, Zhang Wang, Hu Wei, Su Jun, Dai Hengfen, Gu Ping, Huang Xiaohong, Du Xiaoming, Li Ruijuan, Zheng Qiaowei, Lin Xiangsheng, Zhang Yanxia, Zou Lang, Liu Yuxin, Zhang Min, Liu Xiumei, Zhu Zhu, Sun Jianjun, Hong Shanshan, She Weibin, Zhang Jinhua
Department of Pharmacy, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, #18 Daoshan Road, Fuzhou, 350001, China.
Department of Cardiology, Fujian Medical University Union Hospital, Fujian, 350001, China.
Thromb J. 2023 Apr 5;21(1):37. doi: 10.1186/s12959-023-00483-6.
Based on the few available studies on the prognostic benefit of using direct oral anticoagulants (DOACs) after atrial fibrillation (AF) ablation. Therefore, this study aimed to evaluate the prognostic differences between patients who underwent radiofrequency ablation (RFA) and those without RFA taking DOACs.
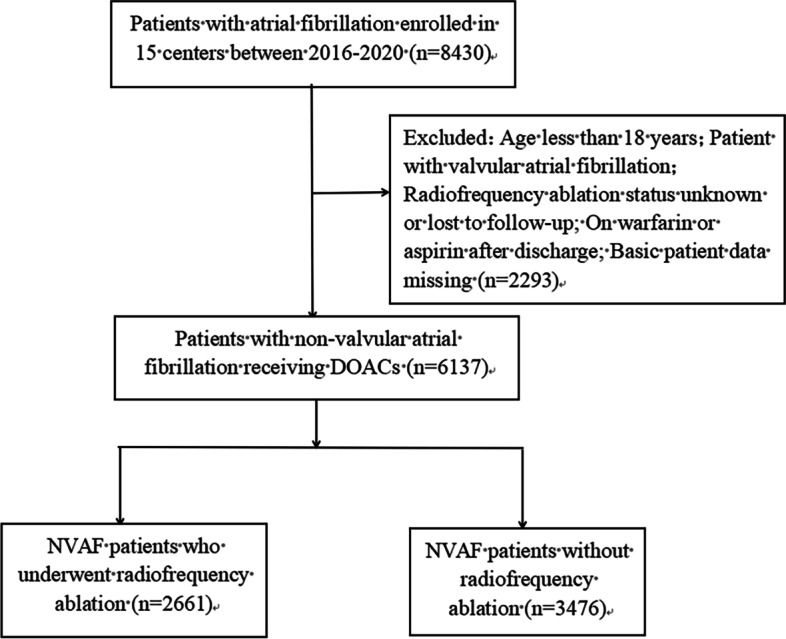
This is a multicenter retrospective cohort study enrolling 6137 patients with non-valvular AF (NVAF) at 15 hospitals in China. Patient information was collected through a mean follow-up of 10 months and medical record queries. Clinical outcomes included major bleeding, total bleeding, thrombosis, all-cause death, and a composite endpoint of bleeding, thrombosis, and all-cause death.
After adjusting for confounders and propensity score matching (PSM), patients with RFA of NVAF had a significantly lower risk of major bleeding [OR 0.278 (95% CI, 0.150-0.515), P<0.001], thrombosis [OR 0.535 (95% CI, 0.316-0.908), P=0.020] and the composite endpoint [ OR 0.835 (95% CI, 0.710-0.982), P=0.029]. In the RFA PSM cohort, dabigatran was associated with reduced all-cause death in patients with RFA of NVAF [OR 0.420 (95% CI, 0.212-0.831), P=0.010]. In the no RFA PSM cohort, rivaroxaban was associated with a reduction in major bleeding [OR 0.521 (95% CI, 0.403-0.673), P<0.001], total bleeding [OR 0.114 (95% CI, 0.049-0.266), P<0.001], and the composite endpoint [OR 0.659 ( 95% CI, 0.535-0.811), P<0.001].
Among patients with NVAF treated with DOACs, RFA was a negative correlate of major bleeding, thrombosis, and composite endpoints but was not associated with total bleeding or all-cause mortality.
基于心房颤动(AF)消融术后使用直接口服抗凝剂(DOACs)的预后益处的现有研究较少。因此,本研究旨在评估接受射频消融(RFA)的患者与未接受RFA但服用DOACs的患者之间的预后差异。
这是一项多中心回顾性队列研究,纳入了中国15家医院的6137例非瓣膜性心房颤动(NVAF)患者。通过平均10个月的随访和病历查询收集患者信息。临床结局包括大出血、总出血、血栓形成、全因死亡以及出血、血栓形成和全因死亡的复合终点。
在调整混杂因素和倾向评分匹配(PSM)后,NVAF接受RFA的患者发生大出血的风险显著降低[比值比(OR)0.278(95%置信区间,0.150 - 0.515),P < 0.001],血栓形成风险降低[OR 0.535(95%置信区间,0.316 - 0.908),P = 0.020],复合终点风险降低[OR 0.835(95%置信区间,0.710 - 0.982),P = 0.029]。在RFA PSM队列中,达比加群与NVAF接受RFA患者的全因死亡降低相关[OR 0.420(95%置信区间,0.212 - 0.831),P = 0.010]。在未接受RFA的PSM队列中,利伐沙班与大出血减少相关[OR 0.521(95%置信区间,0.403 - 0.673),P < 0.001],总出血减少[OR 0.114(95%置信区间,0.049 - 0.266),P < 0.001],以及复合终点减少[OR 0.659(95%置信区间,0.535 - 0.811),P < 0.001]。
在接受DOACs治疗的NVAF患者中,RFA与大出血、血栓形成和复合终点呈负相关,但与总出血或全因死亡率无关。