Sarfati Sacha, Eugène Norbert Misa, Hérault Antoine, Giry Marion, Makké Jade, Grall Maximilien, Savouré Arnaud, Camus Vincent, Alani Mustafa, Tamion Fabienne, Latouche Jean-Baptiste, Girault Christophe
Medical Intensive Care Unit, Normandie Univ, UNIROUEN, UR 3830, CHU Rouen, Medical Intensive Care Unit, Rouen, France.
INSERM U1234, University of Rouen Normandie, Rouen, France.
Front Cardiovasc Med. 2023 Mar 20;10:1132503. doi: 10.3389/fcvm.2023.1132503. eCollection 2023.
CD19-specific chimeric antigen receptor T (CAR-T) cell therapy has recently been shown to improve the prognosis of refractory diffuse large B-cell lymphoma (DLBCL). However, CAR-T cells may induce numerous adverse events, in particular cytokine release syndrome (CRS) which is frequently associated with cardiovascular manifestations. Among the latter, acute pericardial effusion represents less than 1% of cases and cardiac tamponade has only been reported once. The management and outcome of these severe complications are not well established. We report here, a case of cardiac tamponade associated with CRS in a context of CAR-T cell therapy, which required urgent pericardiocentesis.
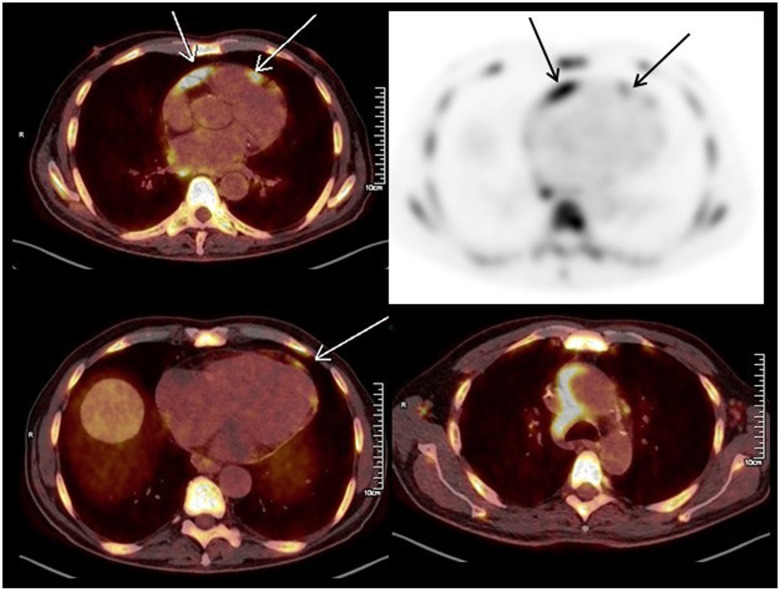
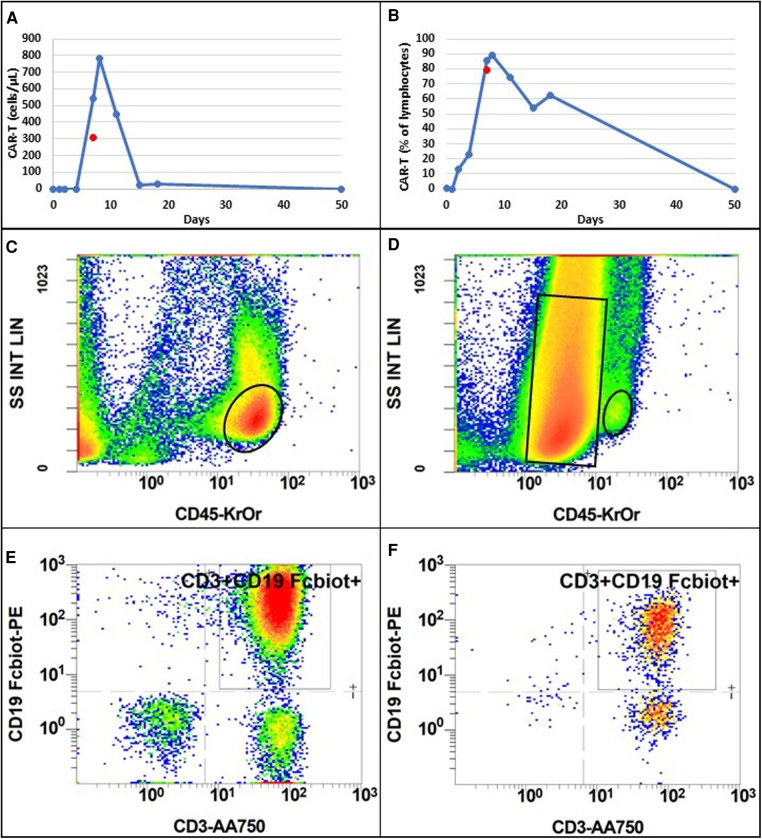
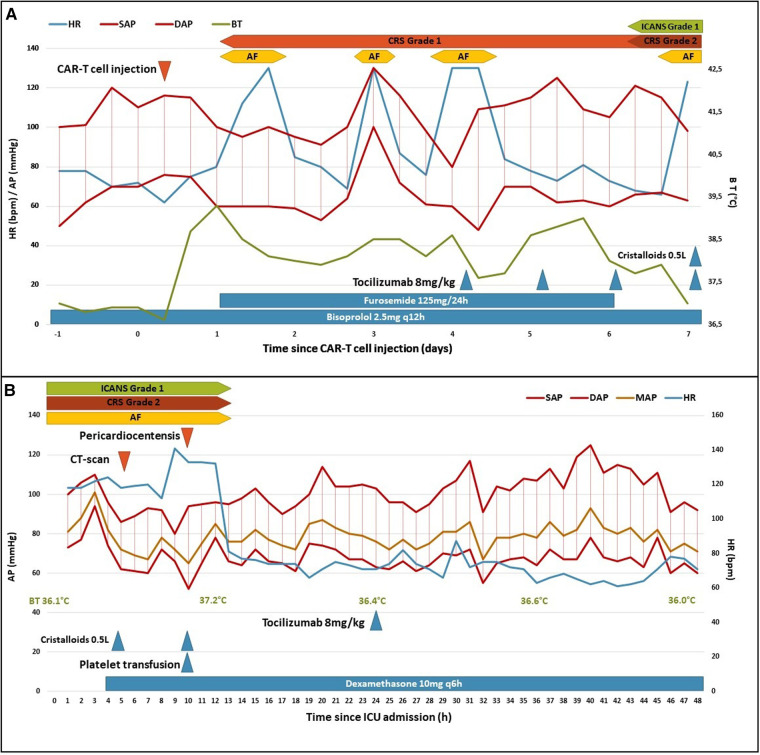
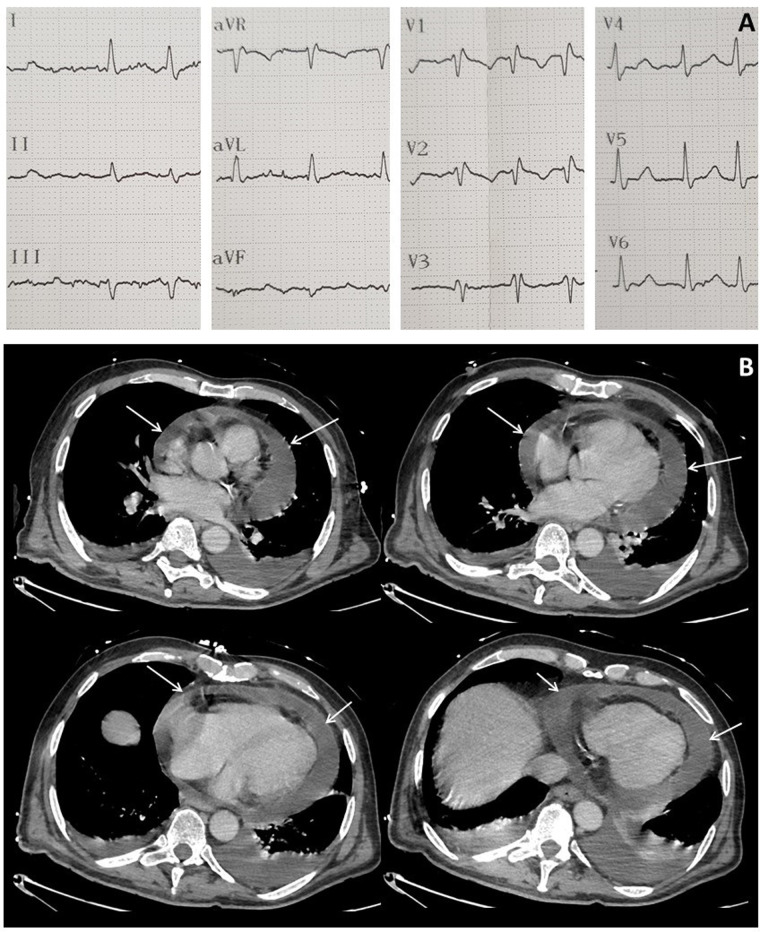
A 65-year-old man with refractory DLBCL was treated with CAR-T cell therapy. He had a history of dilated cardiomyopathy with preserved ejection fraction and transient atrial fibrillation. A pericardial localization of the lymphoma was observed on the second relapse. One day after CAR-T cell infusion the patient was diagnosed with grade 1 CRS. Due to hypotension, he was treated with tocilizumab and dexamethasone, and then transferred to intensive care unit (ICU). Echocardiography performed at ICU admission showed acute pericardial effusion with signs of right ventricular heart failure due to cardiac tamponade. It was decided to perform pericardiocentesis despite grade IV thrombocytopenia in a context of aplasia. Analysis of pericardial fluid showed a large number of lymphoma cells and 73% of CAR-T cells amongst lymphocytes, a level that was similar in blood. Hemodynamic status improved after pericardiocentesis, and no recurrence of pericardial effusion was observed. The presence of a high count of activated CAR-T cells in the pericardial fluid as well as the short interval between CAR-T cells injection and the symptoms appear as potential arguments for a direct action of CAR-T cells in the mechanism of this adverse event. The patient was discharged from ICU after two days and initially exhibited a good response to DLBCL treatment. Unfortunately, he died fifty days after starting CAR-T cell therapy due to a new DLBCL relapse.
Patients with a pericardial localization of DLBCL should be assessed for a risk of cardiac tamponade if receiving CAR-T cell therapy and presenting CRS. In this case, cardiac tamponade seems directly related to CAR-T cell expansion. Pericardiocentesis should be considered as a feasible and effective treatment if the risk of bleeding is well controlled, in association with anti-IL6 and corticosteroids.
最近研究显示,靶向CD19的嵌合抗原受体T(CAR-T)细胞疗法可改善难治性弥漫性大B细胞淋巴瘤(DLBCL)的预后。然而,CAR-T细胞可能引发多种不良事件,尤其是细胞因子释放综合征(CRS),该综合征常伴有心血管表现。其中,急性心包积液的病例占比不到1%,而心脏压塞仅被报道过1次。这些严重并发症的处理方法及预后情况尚无定论。我们在此报告1例在CAR-T细胞治疗过程中发生与CRS相关的心脏压塞病例,该病例需要紧急进行心包穿刺术。
一名65岁难治性DLBCL男性患者接受了CAR-T细胞治疗。他有扩张型心肌病病史,射血分数保留,曾发生过短暂性心房颤动。在第二次复发时观察到淋巴瘤累及心包。CAR-T细胞输注一天后,患者被诊断为1级CRS。由于低血压,他接受了托珠单抗和地塞米松治疗,随后被转入重症监护病房(ICU)。入住ICU时进行的超声心动图检查显示急性心包积液,并伴有因心脏压塞导致的右心室心力衰竭体征。尽管患者处于再生障碍性贫血状态且血小板减少为IV级,但仍决定进行心包穿刺术。心包液分析显示有大量淋巴瘤细胞,淋巴细胞中CAR-T细胞占73%,这一比例与血液中的相似。心包穿刺术后血流动力学状态改善,未观察到心包积液复发。心包液中存在大量活化的CAR-T细胞,以及CAR-T细胞注射与症状出现之间的时间间隔较短,这些似乎都表明CAR-T细胞在这一不良事件的机制中具有直接作用。患者在两天后从ICU出院,最初对DLBCL治疗反应良好。不幸的是,他在开始CAR-T细胞治疗五十天后因DLBCL再次复发而死亡。
对于DLBCL累及心包的患者,如果接受CAR-T细胞治疗并出现CRS,应评估其发生心脏压塞的风险。在本病例中,心脏压塞似乎与CAR-T细胞扩增直接相关。如果出血风险得到良好控制,心包穿刺术应被视为一种可行且有效的治疗方法,并可联合使用抗IL-6药物和皮质类固醇。