Department of Surgery, Sahlgrenska Breast Center, Sahlgrenska University Hospital, Region Västra Götaland, Gothenburg, Sweden.
Department of Clinical Pathology, Institute of Biomedicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Breast Cancer Res. 2023 Apr 6;25(1):36. doi: 10.1186/s13058-023-01632-5.
When ipsilateral multifocal primary breast cancer (IMBC) is detected, standard routine is to evaluate the largest tumor with immunohistochemistry (IHC). As all foci are not routinely characterized, many patients may not receive optimal adjuvant treatment. Here, we assess the clinical relevance of examining at least two foci present in patients with IMBC.
Patients diagnosed and treated for IMBC at Sahlgrenska University Hospital (Gothenburg, Sweden) between 2012 and 2017 were screened. In total, 180 patients with ≥ 2 invasive foci (183 specimens) were assessed with IHC and included in this study. Expression of the estrogen (ER) and progesterone (PR) receptors, Ki67, HER2, and tumor grade were used to determine the molecular surrogate subtypes and discordance among the foci was recorded. An additional multidisciplinary team board was then held to re-assess whether treatment recommendations changed due to discordances in molecular surrogate subtype between the different foci.
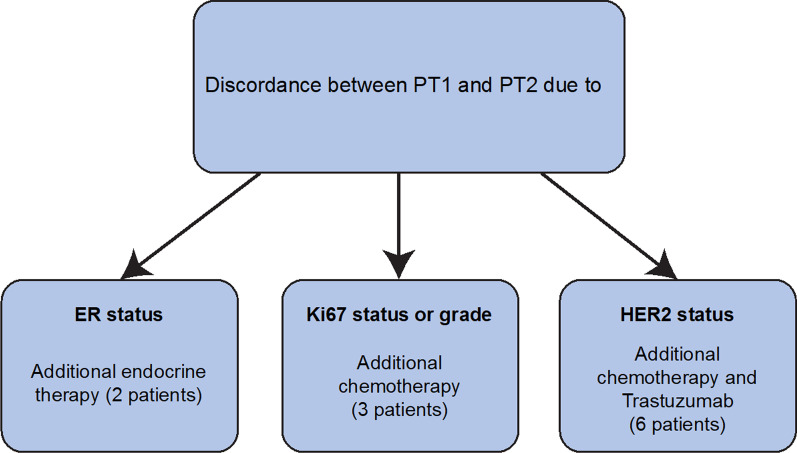
Discordance in ER, PR, HER2, and Ki67 was found in 2.7%, 19.1%, 7.7%, and 16.9% of invasive foci, respectively. Discordance in the molecular surrogate subtypes was found in 48 of 180 (26.7%) patients, which resulted in therapy changes for 11 patients (6.1%). These patients received additional endocrine therapy (n = 2), chemotherapy (n = 3), and combined chemotherapy and trastuzumab (n = 6).
Taken together, when assessing at least two tumor foci with IHC, regardless of shared morphology or tumor grade between the different foci, 6.1% of patients with IMBC were recommended additional adjuvant treatment. A pathologic assessment using IHC of all foci is therefore recommended to assist in individualized treatment decision making.
当同侧多灶原发性乳腺癌(IMBC)被检出时,标准常规是用免疫组织化学(IHC)评估最大肿瘤。由于并非所有病灶都常规进行特征描述,许多患者可能无法接受最佳辅助治疗。在此,我们评估了在 IMBC 患者中检查至少两个病灶的临床相关性。
筛选了在瑞典哥德堡 Sahlgrenska 大学医院(Sahlgrenska University Hospital)诊断和治疗 IMBC 的患者。共有 180 名具有≥2 个浸润性病灶(183 个标本)的患者接受了 IHC 评估并被纳入本研究。使用雌激素(ER)和孕激素(PR)受体、Ki67、HER2 和肿瘤分级来确定分子替代亚型,并记录病灶之间的不一致性。然后,举行了一个额外的多学科团队会议,以重新评估由于不同病灶之间的分子替代亚型的不一致性,治疗建议是否发生变化。
在 180 名浸润性病灶中,分别有 2.7%、19.1%、7.7%和 16.9%的病灶在 ER、PR、HER2 和 Ki67 表达上存在不一致。在 48 名(26.7%)患者中发现了分子替代亚型的不一致,这导致 11 名患者(6.1%)的治疗方案发生了改变。这些患者接受了额外的内分泌治疗(n=2)、化疗(n=3)和化疗联合曲妥珠单抗治疗(n=6)。
总之,当用 IHC 评估至少两个肿瘤病灶时,无论不同病灶之间是否具有共享的形态学或肿瘤分级,6.1%的 IMBC 患者被推荐接受额外的辅助治疗。因此,建议对所有病灶进行 IHC 病理评估,以协助个体化治疗决策。