Department of Cardiac Surgery and ICU, Saudi German Hospital, Dubai, UAE.
Department of Surgery, Kremlim Bicetre Hospital, Paris, France.
J Cardiothorac Surg. 2023 Apr 6;18(1):101. doi: 10.1186/s13019-023-02229-x.
There is still ongoing debate about the benefits of mini-thoracotomy (MTH) approach in mitral valve surgery in comparison with complete sternotomy (STER). This study aims to update the current evidence with mortality as primary end point.
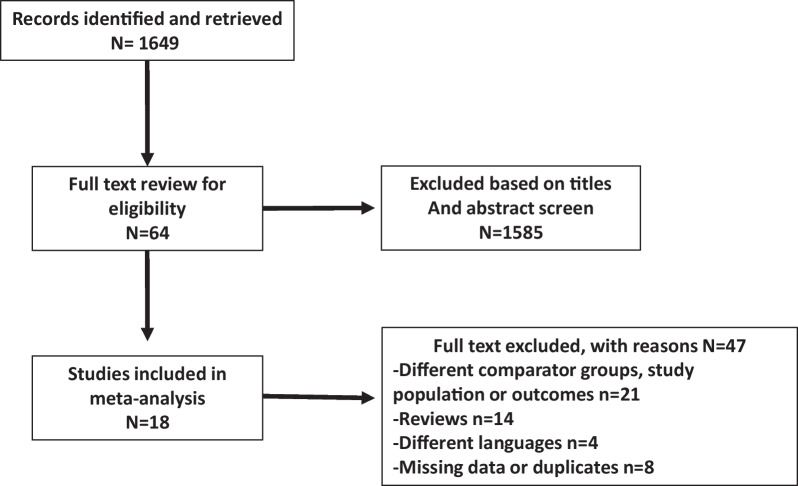
The MEDLINE and EMBASE databases were searched through June 2022. Two randomized studies and 16 propensity score matched studies published from 2011 to 2022 were included with a total of 12,997 patients operated on from 2005 (MTH: 6467, STER: 6530). Data regarding early mortality, stroke, reoperation for bleeding, new renal failure, new onset of atrial fibrillation, need of blood transfusion, prolonged ventilation, wound infection, time-related outcomes (cross clamp time, cardiopulmonary bypass time, ventilation time, length of intensive care unit stay, length of hospital stay), midterm mortality and reoperation, and costs were extracted and submitted to a meta-analysis using weighted random effects modeling.
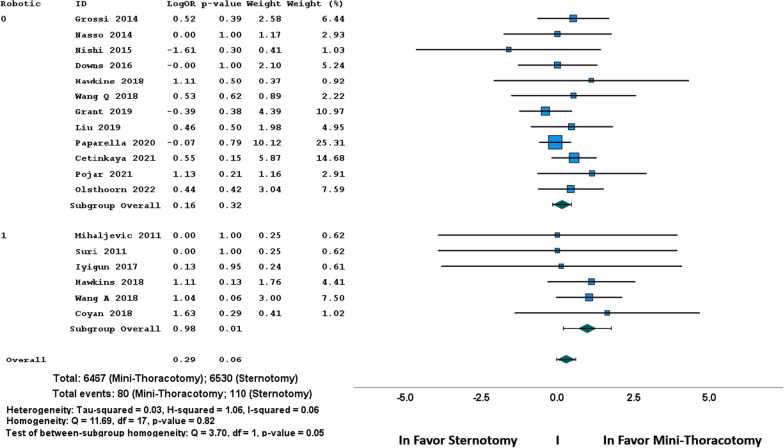
The incidence of early mortality, stroke, reoperation for bleeding and prolonged ventilation were similar, all in the absence of heterogeneity. However, the sub-group analysis showed a significant OR in favor of MTH when robotic enhancement was used. New renal failure (OR 1.67, 95% CI 1.06-2.62, p = 0.03), new onset of atrial fibrillation (OR 1.31, 95% CI 1.15-1.51, p = 0.001) and the need of blood transfusion (OR 1.77, 95% CI 1.39-2.27, p = 0.001) were significantly lower in MTH group. Regarding time-related outcomes, there was evidence for important heterogeneity of treatment effect among the studies. Operative times were longer in MTH: differences in means were 20.7 min for cross clamp time (95% CI 14.9-26.4, p = 0.001), 36.8 min for CPB time (95% CI 29.8-43.9, p = 0.001) and 37.7 min for total operative time (95% CI 19.6-55.8, p < 0.001). There was no significant difference in ventilation duration; however, the differences in means showed significantly shorter ICU stay and hospital stay after MTH compared to STER: - 0.6 days (95% CI - 1.1/- 0.21, p = 0.001) and - 1.88 days (95% CI - 2.72/- 1.05, p = 0.001) respectively, leading to a significant lower hospital cost after MTH compared to STER with difference in means - 4528 US$ (95% CI - 8725/- 326, p = 0.03). The mid-term mortality was significantly higher after STER compared to MTH: OR = 1.50, 1.09-2.308 (95% CI), p = 0.01; the rate of mid-term reoperation was reported similar in MTH and STER: OR = 0.76, 0.50-1.15 (95% CI), p = 0.19.
The present meta-analysis confirms that the MTH approach for mitral valve disease remains associated with prolonged operative times, but it is beneficial in terms of reduced postoperative complications (renal failure, atrial fibrillation, blood transfusion, wound infection), length of stay in ICU and in hospitalization, with finally a reduction in global cost. MTH approach appears associated with a significant reduction of postoperative mortality that must be confirmed by large randomized study.
在二尖瓣手术中,微创小切口(MTH)与完全胸骨切开术(STER)相比的优势仍存在争议。本研究旨在更新目前以死亡率为主要终点的证据。
通过 2022 年 6 月检索 MEDLINE 和 EMBASE 数据库。纳入了 2011 年至 2022 年发表的 2 项随机研究和 16 项倾向评分匹配研究,共纳入了 2005 年接受手术治疗的 12997 例患者(MTH:6467 例,STER:6530 例)。提取并提交了有关早期死亡率、中风、再次出血手术、新发肾衰竭、新发心房颤动、输血需要、延长通气、伤口感染、时间相关结局(体外循环时间、心肺转流时间、通气时间、重症监护病房住院时间、住院时间)、中期死亡率和再次手术以及成本的数据,并使用加权随机效应模型进行荟萃分析。
早期死亡率、中风、再次出血手术和延长通气的发生率相似,均无异质性。然而,亚组分析显示,当使用机器人增强时,MTH 具有显著的优势比。新发肾衰竭(OR 1.67,95%CI 1.06-2.62,p=0.03)、新发心房颤动(OR 1.31,95%CI 1.15-1.51,p=0.001)和输血需要(OR 1.77,95%CI 1.39-2.27,p=0.001)在 MTH 组显著降低。在时间相关结局方面,研究之间存在治疗效果的重要异质性。MTH 组的手术时间更长:夹闭时间的差异为 20.7 分钟(95%CI 14.9-26.4,p=0.001),CPB 时间的差异为 36.8 分钟(95%CI 29.8-43.9,p=0.001),总手术时间的差异为 37.7 分钟(95%CI 19.6-55.8,p<0.001)。通气时间无显著差异;然而,与 STER 相比,MTH 后 ICU 停留时间和住院时间明显缩短:-0.6 天(95%CI -1.1/-0.21,p=0.001)和-1.88 天(95%CI -2.72/-1.05,p=0.001),导致 MTH 后住院费用显著低于 STER,差异为-4528 美元(95%CI -8725/-326,p=0.03)。与 MTH 相比,STER 中期死亡率明显更高:OR=1.50,1.09-2.308(95%CI),p=0.01;MTH 和 STER 中期再次手术率报告相似:OR=0.76,0.50-1.15(95%CI),p=0.19。
本荟萃分析证实,二尖瓣疾病的 MTH 方法仍然与手术时间延长有关,但在减少术后并发症(肾衰竭、心房颤动、输血、伤口感染)、ICU 住院时间和住院时间、最终降低整体成本方面是有益的。MTH 方法似乎与术后死亡率的显著降低有关,但这需要通过大型随机研究来证实。