Department of Community Medicine & School of Public Health, Postgraduate Institute of Medical Education & Research, Chandigarh, India.
Department of Internal Medicine, Postgraduate Institute of Medical Education & Research, Chandigarh, India.
Indian J Med Res. 2022 Jun;156(6):705-714. doi: 10.4103/ijmr.IJMR_806_20.
BACKGROUND & OBJECTIVES: The World Health Organisation recommended immediate initiation of antiretroviral therapy (ART) in all adult human immunodeficiency virus (HIV) patients regardless of their CD4 cell count. This study was undertaken to ascertain the cost-effectiveness of implementation of these guidelines in India.
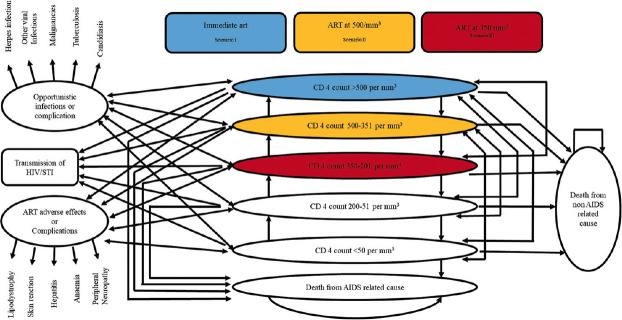
A Markov model was developed to assess the lifetime costs and health outcomes of three scenarios for initiation of ART treatment at varying CD4 cell count <350/mm, <500/mm and test and treat using health system perspective using life-time horizon. A few input parameters for this model namely, transition probabilities from one stage to another stage of HIV and incidence rates of TB were calculated from the data of Centre of Excellence for HIV treatment and care, Chandigarh; whereas, other parameters were obtained from the published literature. Total HIV-related deaths averted, HIV infections averted and incremental cost-effectiveness ratio per quality adjusted life years (QALYs) gained were calculated.
Test and treat intervention slowed down the progression of disease and averted 18,386 HIV-related deaths, over lifetime horizon. It also averted 16,105 new HIV infections and saved 343,172 QALYs as compared to the strategy of starting ART at CD4 cell count of 500/mm. Incremental cost per QALY gained for the immediate initiation of ART as compared to ART at CD4 cell count of 500/mm and 350/mm was ₹ 46,599 and 80,050, respectively at reported rates of adherence to the therapy.
INTERPRETATION & CONCLUSIONS: Immediate ART (test and treat) is highly cost-effective strategy over the past criteria of delayed therapy in India. Cost-effectiveness of this policy is largely because of reduction in the transmission of HIV.
世界卫生组织建议所有成人人类免疫缺陷病毒(HIV)患者无论其 CD4 细胞计数如何,都应立即开始抗逆转录病毒治疗(ART)。本研究旨在确定在印度实施这些指南的成本效益。
我们建立了一个马尔可夫模型,以评估在不同 CD4 细胞计数<350/mm、<500/mm 和根据检测结果进行治疗的情况下实施 ART 治疗方案的三种情况的终生成本和健康结果,从卫生系统的角度使用终生时间范围进行评估。该模型的一些输入参数,如从 HIV 的一个阶段到另一个阶段的转移概率和结核病的发病率,是根据昌迪加尔艾滋病治疗和护理卓越中心的数据计算得出的;而其他参数则是从已发表的文献中获得的。计算了避免的总 HIV 相关死亡人数、避免的 HIV 感染人数以及每获得一个质量调整生命年(QALY)的增量成本效益比。
测试和治疗干预措施减缓了疾病的进展,在整个生命过程中避免了 18386 例 HIV 相关死亡。与在 CD4 细胞计数为 500/mm 时开始 ART 的策略相比,它还避免了 16105 例新的 HIV 感染,并节省了 343172 个 QALYs。与在 CD4 细胞计数为 500/mm 和 350/mm 时开始 ART 相比,立即开始 ART 的增量成本效益比分别为每 QALY 获得 46599 卢比和 80050 卢比,在报告的治疗依从率下。
在印度,与过去延迟治疗的标准相比,立即开始 ART(测试和治疗)是一种极具成本效益的策略。该政策的成本效益在很大程度上是因为减少了 HIV 的传播。