Maddali Manoj V, Dowdy David W, Gupta Amita, Shah Maunank
Division of Infectious Diseases, Department of Medicine, School of Medicine, Johns Hopkins University, Baltimore, MD, USA.
Department of Epidemiology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA.
J Int AIDS Soc. 2015 Oct 1;18(1):20217. doi: 10.7448/IAS.18.1.20217. eCollection 2015.
Recent WHO guidance advocates for early antiretroviral therapy (ART) initiation at higher CD4 counts to improve survival and reduce HIV transmission. We sought to quantify how the cost-effectiveness and epidemiological impact of early ART strategies in India are affected by attrition throughout the HIV care continuum.
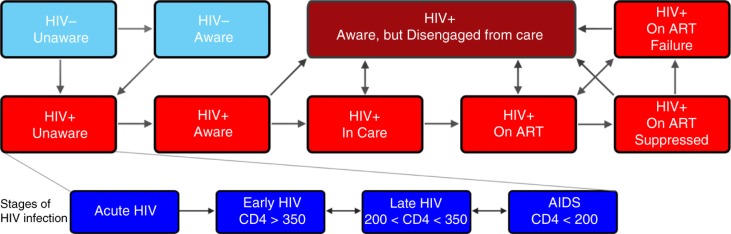
We constructed a dynamic compartmental model replicating HIV transmission, disease progression and health system engagement among Indian adults. Our model of the Indian HIV epidemic compared implementation of early ART initiation (i.e. initiation above CD4 ≥350 cells/mm(3)) with delayed initiation at CD4 ≤350 cells/mm(3); primary outcomes were incident cases, deaths, quality-adjusted-life-years (QALYs) and costs over 20 years. We assessed how costs and effects of early ART initiation were impacted by suboptimal engagement at each stage in the HIV care continuum.
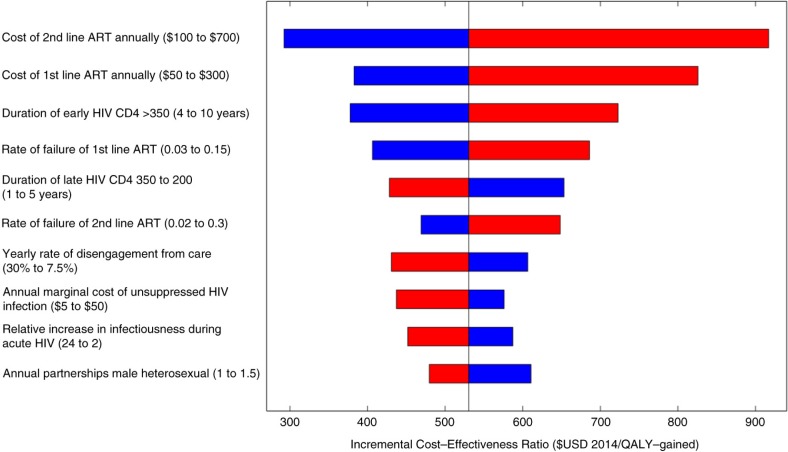
Assuming "idealistic" engagement in HIV care, early ART initiation is highly cost-effective ($442/QALY-gained) compared to delayed initiation at CD4 ≤350 cells/mm(3) and could reduce new HIV infections to <15,000 per year within 20 years. However, when accounting for realistic gaps in care, early ART initiation loses nearly half of potential epidemiological benefits and is less cost-effective ($530/QALY-gained). We project 1,285,000 new HIV infections and 973,000 AIDS-related deaths with deferred ART initiation with current levels of care-engagement in India. Early ART initiation in this continuum resulted in 1,050,000 new HIV infections and 883,000 AIDS-related deaths, or 18% and 9% reductions (respectively), compared to current guidelines. Strengthening HIV screening increases benefits of earlier treatment modestly (1,001,000 new infections; 22% reduction), while improving retention in care has a larger modulatory impact (676,000 new infections; 47% reduction).
Early ART initiation is highly cost-effective in India but only has modest epidemiological benefits at current levels of care-engagement. Improved retention in care is needed to realize the full potential of earlier treatment.
世界卫生组织(WHO)近期发布的指南提倡在更高的CD4细胞计数时尽早开始抗逆转录病毒治疗(ART),以提高生存率并减少HIV传播。我们试图量化在印度,贯穿HIV治疗全程的失访情况如何影响早期ART策略的成本效益和流行病学影响。
我们构建了一个动态的 compartments 模型,用以复制印度成年人中的HIV传播、疾病进展以及卫生系统参与情况。我们的印度HIV流行模型比较了早期ART启动(即CD4≥350个细胞/mm³时启动)与CD4≤350个细胞/mm³时延迟启动的实施情况;主要结局指标为20年内的新发病例、死亡人数、质量调整生命年(QALYs)和成本。我们评估了HIV治疗全程中每个阶段次优参与情况如何影响早期ART启动的成本和效果。
假设在HIV治疗中存在“理想”的参与情况,与CD4≤350个细胞/mm³时延迟启动相比,早期ART启动具有很高的成本效益(每获得一个QALY成本为442美元),并且在20年内可将每年的新HIV感染病例减少至<15,000例。然而,考虑到实际的治疗差距时,早期ART启动会损失近一半的潜在流行病学益处,且成本效益降低(每获得一个QALY成本为530美元)。按照印度目前的治疗参与水平,我们预计延迟ART启动会导致128.5万例新的HIV感染和97.3万例与艾滋病相关的死亡。与现行指南相比,在此治疗全程中早期ART启动导致105万例新的HIV感染和88.3万例与艾滋病相关的死亡,分别减少了18%和9%。加强HIV筛查适度增加了早期治疗的益处(100.1万例新感染;减少22%),而改善治疗留存率则具有更大的调节作用(67.6万例新感染;减少47%)。
在印度,早期ART启动具有很高的成本效益,但在目前的治疗参与水平下仅具有适度的流行病学益处。需要提高治疗留存率以充分发挥早期治疗的潜力。