Department of Medicine IV, Faculty of Medicine, University Freiburg Medical Centre, University of Freiburg, Hugstetter Street 55, Freiburg, 79106, Germany.
Department of Medicine II, Division of Infectious Diseases, Faculty of Medicine, University Freiburg Medical Centre, University of Freiburg, Freiburg, Germany.
BMC Nephrol. 2023 Apr 15;24(1):99. doi: 10.1186/s12882-023-03154-w.
Despite vaccination coronavirus disease 2019 (COVID-19)-associated mortality caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) remains high in kidney transplant recipients. Nirmatrelvir is a protease inhibitor with activity against SARS-CoV-2. Nirmatrelvir reduces the risk for mortality and hospitalization, which is approved for treating adults at risk for severe disease. Nirmatrelvir is metabolized by the cytochrome P-450 (CYP) 3A4 isozyme CYP3A4 and is therefore co-administered with the irreversible CYP3A4 inhibitor ritonavir, which results in a drug interaction with tacrolimus. A limited number of patients with nirmatrelvir/ritonavir and tacrolimus therapy after kidney transplantation have been reported to date. It has been reported that tacrolimus was paused during the five-day nirmatrelvir/ritonavir therapy and subtherapeutic tacrolimus levels were observed after finishing nirmatrelvir/ritonavir in two patients. Therefore, optimization of tacrolimus dosing is urgently needed in transplant recipients receiving nirmatrelvir/ritonavir treatment.
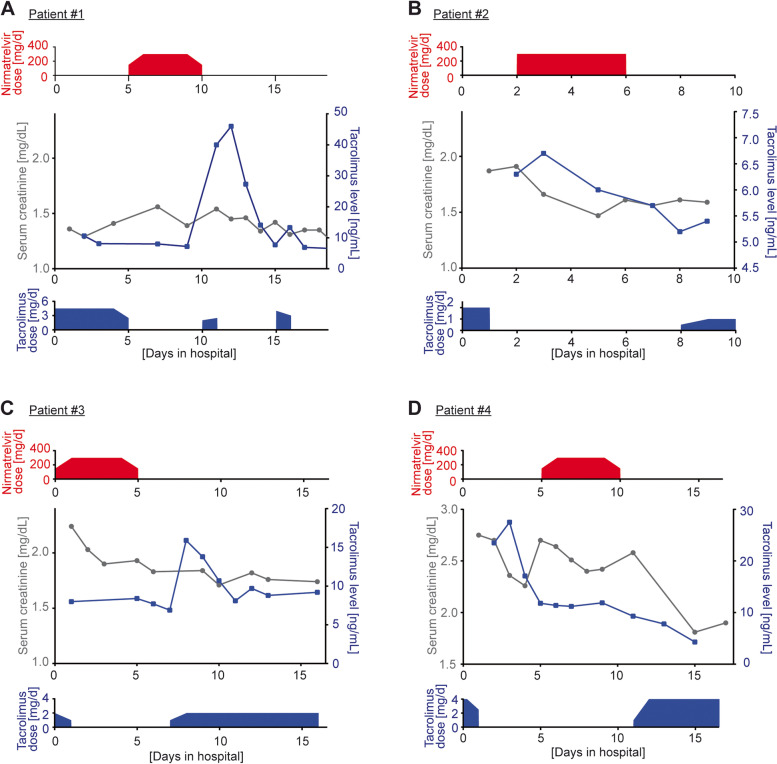
Here, we present our first-hand experience with four patients receiving tacrolimus therapy following kidney transplantation and nirmatrelvir/ritonavir therapy due to COVID-19. Tacrolimus was paused during nirmatrelvir/ritonavir therapy in all patients, which resulted in stable therapeutic tacrolimus levels. Tacrolimus was continued directly after finishing nirmatrelvir/ritonavir to avoid subtherapeutic levels in the first patient treated. This patient received his usual tacrolimus maintenance dose, which resulted in toxic levels. Based on this observation, tacrolimus therapy was continued 24 h after finishing nirmatrelvir/ritonavir treatment at a reduced dose in the subsequent patients. In these patients, therapeutic to supratherapeutic tacrolimus levels were observed despite the therapeutic break and dose reduction.
Based on altered CYP3A4 metabolism, tacrolimus levels have to be closely monitored after treatment with nirmatrelvir/ritonavir. Our study suggests that tacrolimus treatment should be paused during nirmatrelvir/ritonavir medication and be continued 24 h after completing nirmatrelvir/ritonavir therapy at a reduced dose and under close monitoring. Based on the limited number of patients in this study, results must be interpreted with caution.
尽管接种疫苗,由严重急性呼吸系统综合症冠状病毒 2(SARS-CoV-2)引起的 2019 冠状病毒病(COVID-19)相关死亡率在肾移植受者中仍然很高。奈玛特韦是一种针对 SARS-CoV-2 的蛋白酶抑制剂。奈玛特韦降低了死亡率和住院风险,已被批准用于治疗有重症疾病风险的成年人。奈玛特韦由细胞色素 P-450(CYP)3A4 同工酶 CYP3A4 代谢,因此与不可逆的 CYP3A4 抑制剂利托那韦联合给药,这导致与他克莫司发生药物相互作用。迄今为止,已报告了少数接受奈玛特韦/利托那韦和肾移植后他克莫司治疗的患者。据报道,在五天的奈玛特韦/利托那韦治疗期间暂停他克莫司,并且在两名患者完成奈玛特韦/利托那韦后观察到他克莫司低于治疗水平。因此,接受奈玛特韦/利托那韦治疗的移植受者急需优化他克莫司的剂量。
在这里,我们介绍了我们在四例肾移植后 COVID-19 患者接受奈玛特韦/利托那韦治疗后接受他克莫司治疗的第一手经验。所有患者在奈玛特韦/利托那韦治疗期间暂停他克莫司,结果稳定了治疗性他克莫司水平。在第一个接受治疗的患者中,在完成奈玛特韦/利托那韦后直接继续使用他克莫司,以避免低于治疗水平。该患者接受了常规的他克莫司维持剂量,结果出现了毒性水平。基于这一观察结果,在随后的患者中,在完成奈玛特韦/利托那韦治疗后 24 小时,以较低剂量继续他克莫司治疗。尽管有治疗中断和剂量减少,但这些患者仍观察到治疗性至超治疗性他克莫司水平。
基于 CYP3A4 代谢的改变,在使用奈玛特韦/利托那韦治疗后必须密切监测他克莫司水平。我们的研究表明,在奈玛特韦/利托那韦药物治疗期间应暂停他克莫司治疗,并在完成奈玛特韦/利托那韦治疗后 24 小时,以较低剂量继续治疗并密切监测。基于本研究中患者数量有限,结果必须谨慎解释。