Department of Cardiology, The Second People's Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Hefei, 230011, Anhui, China.
The Fifth School of Clinical Medicine, Anhui Medical University, Hefei, 230032, Anhui, China.
BMC Cardiovasc Disord. 2023 Apr 17;23(1):198. doi: 10.1186/s12872-023-03214-x.
Patients with acute ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) are at high risk of major adverse cardiovascular events (MACE) despite timely treatment. This study aimed to investigate the independent predictors and their predictive value of in-hospital MACE after primary PCI in patients with acute STEMI under the China chest pain center (standard center) treatment system.
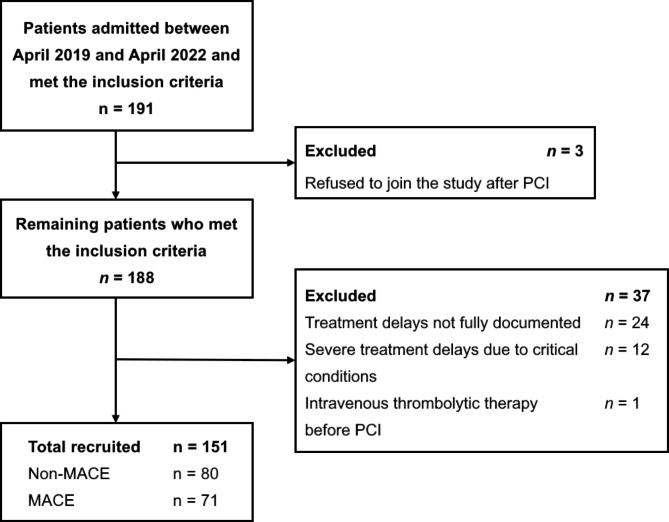
We performed a single-center, retrospective study of 151 patients with acute STEMI undergoing primary PCI. All patients were treated under the China chest pain center (standard center) treatment system. The data collected included general data, vital signs, auxiliary examination results, data related to interventional therapy, and various treatment delays. The primary endpoint was the in-hospital MACE defined as the composite of all-cause death, stroke, nonfatal recurrent myocardial infarction, new-onset heart failure, and malignant arrhythmias.
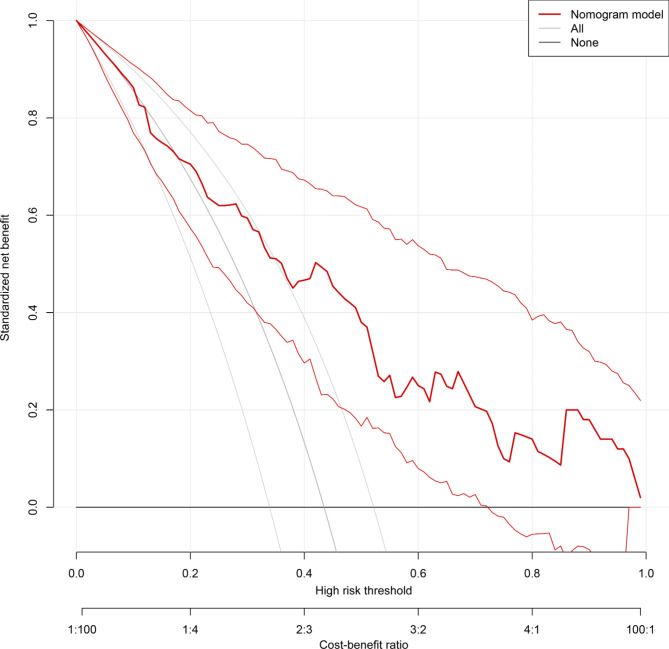
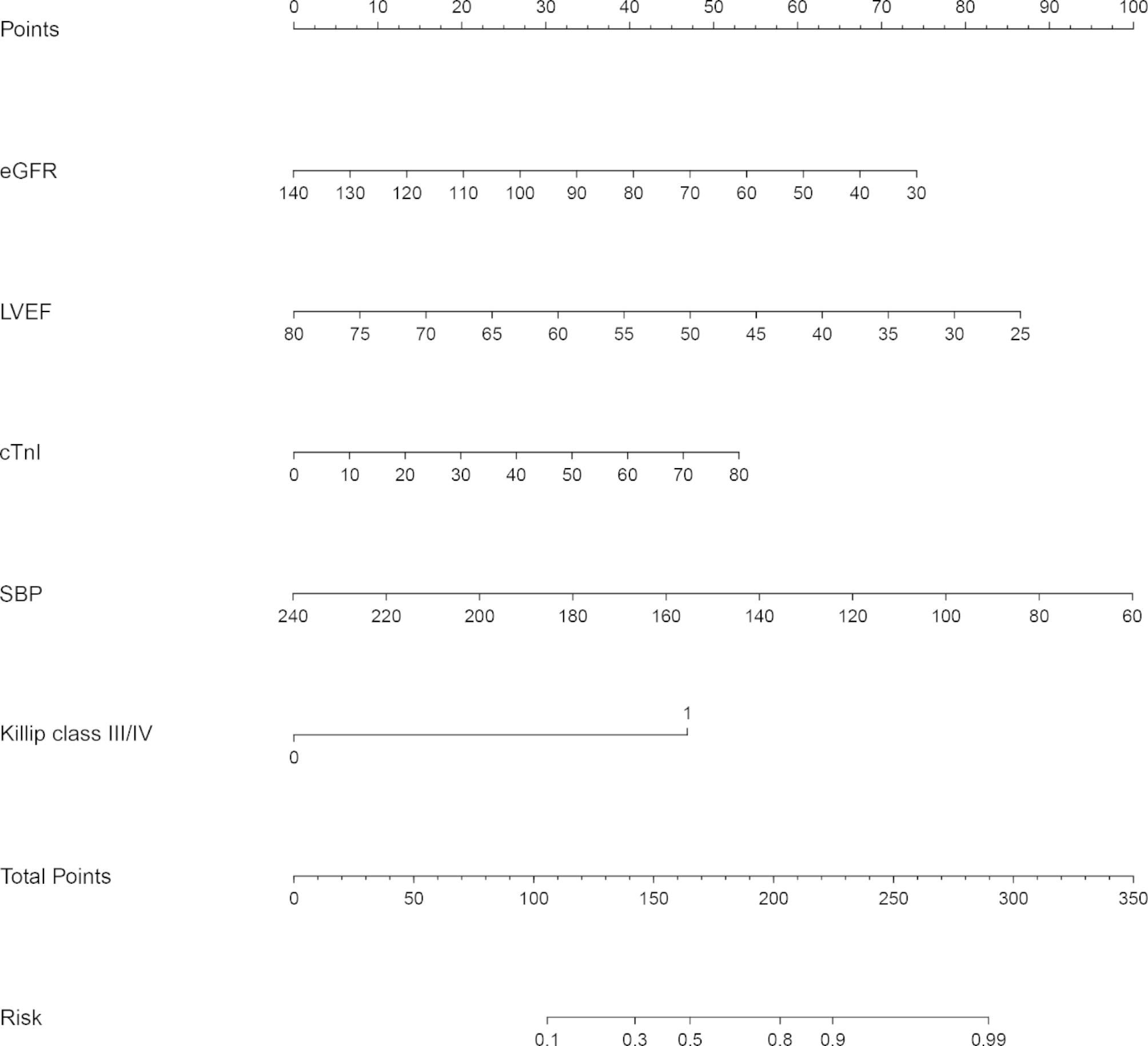
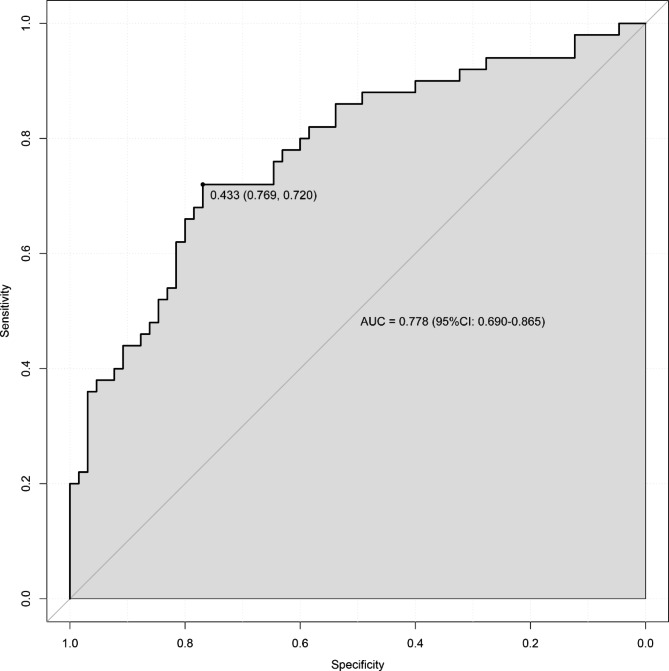
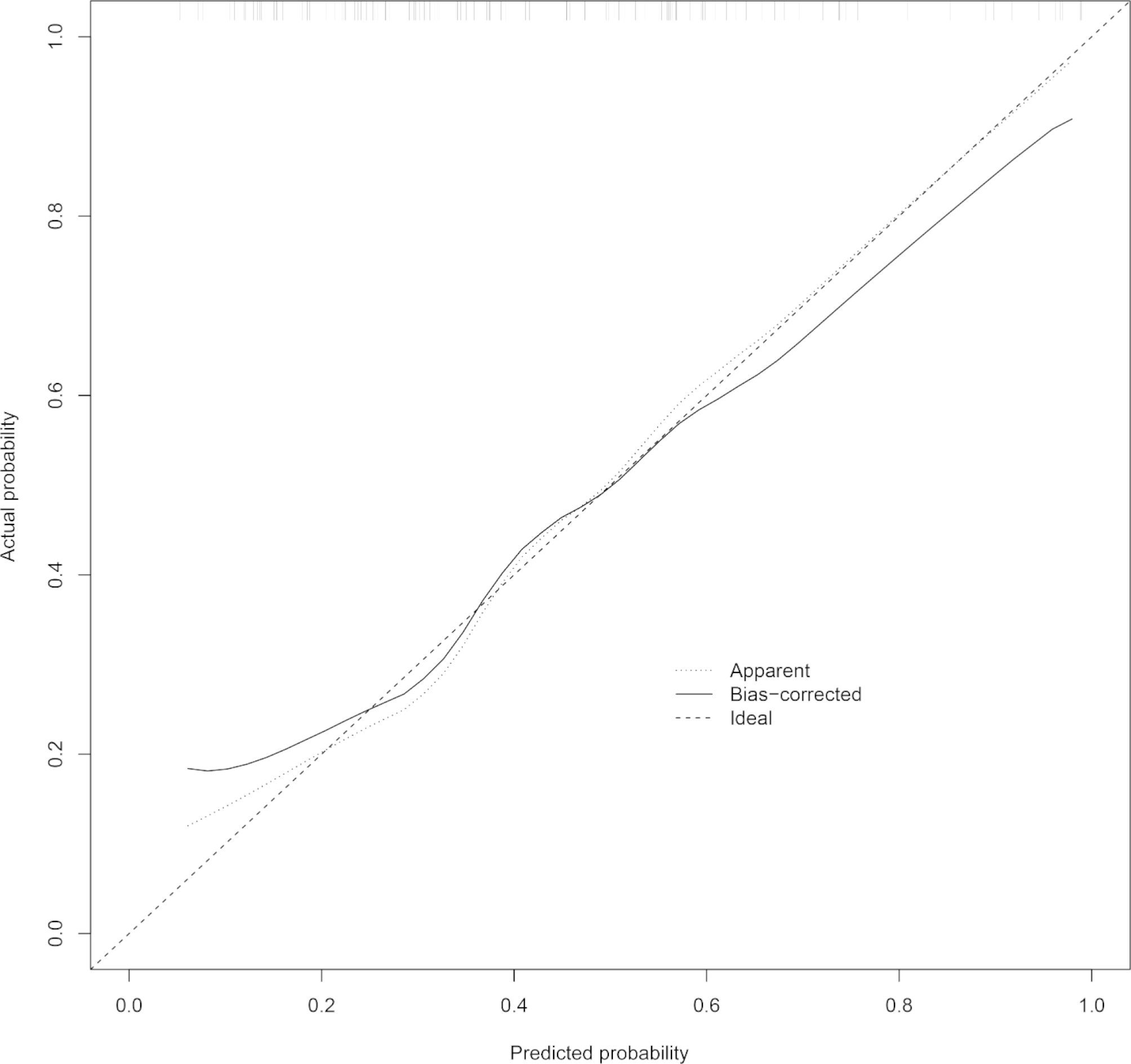
In-hospital MACE occurred in 71 of 151 patients with acute STEMI undergoing primary PCI. Logistic regression analysis showed that age, cardiac troponin I (cTnI), serum creatinine (sCr), multivessel coronary artery disease, and Killip class III/IV were risk factors for in-hospital MACE, whereas estimated glomerular filtration rate (eGFR), left ventricular ejection fraction (LVEF), systolic blood pressure (SBP), diastolic blood pressure (DBP), were protective factors, with eGFR, LVEF, cTnI, SBP, and Killip class III/IV being independent predictors of in-hospital MACE. The prediction model had good discrimination with an area under the curve = 0. 778 (95%CI: 0.690-0.865). Good calibration and clinical utility were observed through the calibration and decision curves, respectively.
Our data suggest that eGFR, LVEF, cTnI, SBP, and Killip class III/IV independently predict in-hospital MACE after primary PCI in patients with acute STEMI, and the prediction model constructed based on the above factors could be useful for individual risk assessment and early management guidance.
尽管接受了及时的治疗,急性 ST 段抬高型心肌梗死(STEMI)患者行直接经皮冠状动脉介入治疗(PCI)后仍存在发生主要不良心血管事件(MACE)的高风险。本研究旨在探讨在中国胸痛中心(标准中心)治疗体系下接受直接 PCI 的急性 STEMI 患者住院期间发生 MACE 的独立预测因素及其预测价值。
我们对 151 例接受直接 PCI 的急性 STEMI 患者进行了单中心回顾性研究。所有患者均在中国胸痛中心(标准中心)治疗体系下接受治疗。收集的资料包括一般资料、生命体征、辅助检查结果、介入治疗相关资料以及各种治疗延误情况。主要终点为住院期间 MACE,定义为全因死亡、卒死、非致死性再发心肌梗死、新发心力衰竭和恶性心律失常的复合终点。
151 例接受直接 PCI 的急性 STEMI 患者中,71 例发生住院期间 MACE。Logistic 回归分析显示,年龄、肌钙蛋白 I(cTnI)、血清肌酐(sCr)、多支血管病变和 Killip 分级Ⅲ/Ⅳ是住院期间 MACE 的危险因素,而估算肾小球滤过率(eGFR)、左心室射血分数(LVEF)、收缩压(SBP)、舒张压(DBP)是保护因素,其中 eGFR、LVEF、cTnI、SBP 和 Killip 分级Ⅲ/Ⅳ是住院期间 MACE 的独立预测因素。该预测模型的曲线下面积为 0.778(95%CI:0.690-0.865),具有良好的区分度。通过校准和决策曲线分别观察到良好的校准度和临床实用性。
本研究数据表明,eGFR、LVEF、cTnI、SBP 和 Killip 分级Ⅲ/Ⅳ独立预测急性 STEMI 患者直接 PCI 后住院期间的 MACE,基于上述因素构建的预测模型可用于个体风险评估和早期管理指导。