School of Nursing, Shanghai University of Traditional Chinese Medicine, Shanghai, People's Republic of China.
Clinical Center for Intelligent Rehabilitation Research, Shanghai YangZhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center), School of Medicine, Tongji University, Shanghai, People's Republic of China.
Clin Interv Aging. 2023 Apr 18;18:629-638. doi: 10.2147/CIA.S399996. eCollection 2023.
Impaired left ventricular (LV) relaxation is indicative of grade I diastolic dysfunction, which is mainly assessed by late diastolic transmitral flow velocity (E/A ratio). Although the E/A ratio has important diagnostic and prognostic implications with cardiac outcomes, the causal link between abnormal E/A ratio and left ventricle remodeling (LV remodeling) remains unclear.
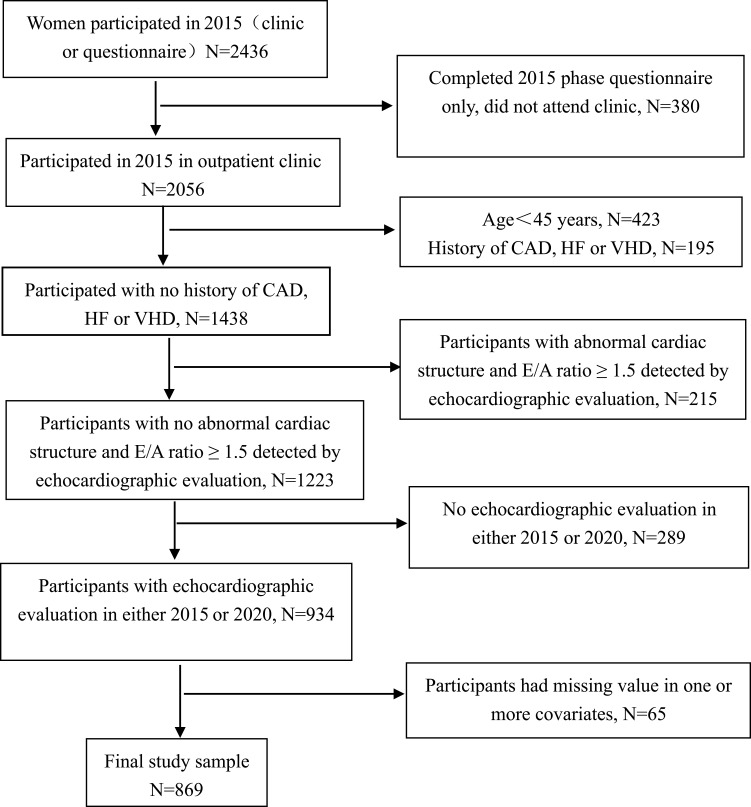
A longitudinal analysis of 869 eligible women aged ≥45 years, who had received echocardiography scans as well as 5-year follow-up assessments between 2015 and 2020. Women with pre-existing cardiac abnormalities including grade II/III diastolic dysfunction as diagnosed by echocardiography, or structural heart disease were excluded. E/A abnormality was defined as baseline E/A ratio <0.8. The classification of LV remodeling was based on the measurements of left ventricular mass index (LVMI) and relative wall thickness (RWT). Logistic and linear regression models were used.
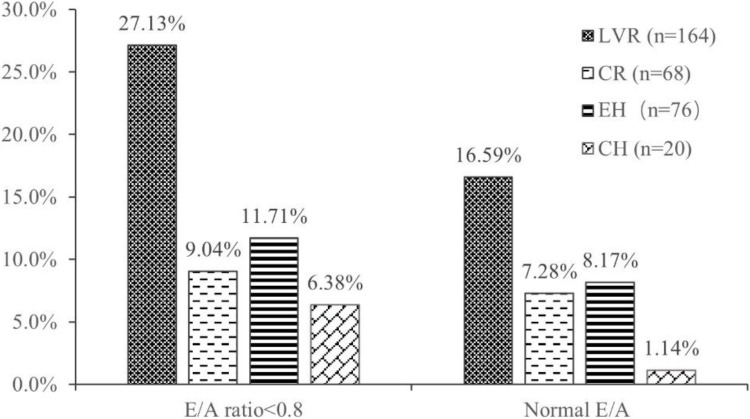
Among the 869 women (60.71±10.01 years), 164 (18.9%) had developed LV remodeling after the 5-year follow-up. The proportion of women with E/A abnormality versus non-abnormality was also significantly different (27.13% vs 16.59%, P=0.007). Multivariable-adjusted regression models showed that E/A abnormality (OR: 4.14, 95%Cl:1.80-9.20, P=0.009) was significantly associated with higher risk of concentric hypertrophy (CH) after follow-up. No such association was found in either concentric remodeling (CR) or eccentric hypertrophy (EH). Higher baseline E/A ratio was correlated with lower ΔRWT during the 5-year follow-up (β=-0.006 m/s, 95% CI: -0.012 to -0.002, P=0.025), which was independent of demographics and biological factors.
E/A abnormality is associated with a higher risk of CH. Higher baseline E/A ratio may be associated with decreased relative changes in RWT.
左心室(LV)舒张功能障碍提示为 I 级舒张功能障碍,主要通过舒张晚期二尖瓣血流速度(E/A 比值)进行评估。尽管 E/A 比值与心脏结局的诊断和预后具有重要意义,但异常 E/A 比值与左心室重构(LV 重构)之间的因果关系仍不清楚。
对 2015 年至 2020 年期间接受超声心动图检查并进行了 5 年随访评估的 869 名年龄≥45 岁的合格女性进行了纵向分析。排除了先前存在心脏异常(包括超声心动图诊断的 II/III 级舒张功能障碍或结构性心脏病)的女性。E/A 异常定义为基线 E/A 比值<0.8。LV 重构的分类基于左心室质量指数(LVMI)和相对壁厚度(RWT)的测量。采用逻辑回归和线性回归模型。
在 869 名女性(60.71±10.01 岁)中,有 164 名(18.9%)在 5 年随访后出现 LV 重构。E/A 异常与非异常的女性比例也有显著差异(27.13%比 16.59%,P=0.007)。多变量调整的回归模型显示,E/A 异常(OR:4.14,95%CI:1.80-9.20,P=0.009)与随访后发生向心性肥厚(CH)的风险显著增加相关。在向心性重构(CR)或偏心性肥厚(EH)中未发现这种相关性。较高的基线 E/A 比值与 5 年随访期间的ΔRWT 呈负相关(β=-0.006 m/s,95%CI:-0.012 至-0.002,P=0.025),这与人口统计学和生物学因素无关。
E/A 异常与 CH 的风险增加相关。较高的基线 E/A 比值可能与 RWT 的相对变化减少有关。