Heart Institute, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea.
Division of Cardiology, Department of Internal Medicine, Soonchunhyang University Hospital, Soonchunhyang University College of Medicine, 170, Jomaru-ro, Bucheon-si, Gyeonggi-do, 14584, Republic of Korea.
BMC Cardiovasc Disord. 2023 Apr 25;23(1):209. doi: 10.1186/s12872-023-03236-5.
The clinical benefits and risks of anticoagulation therapy in patients with chronic kidney disease (CKD) are still inconclusive. We describe the outcomes of patients with atrial fibrillation (AF) after anticoagulation therapy according to differences in creatinine clearance (CrCl). We also aimed to determine the patients who could benefit from anticoagulation therapy.
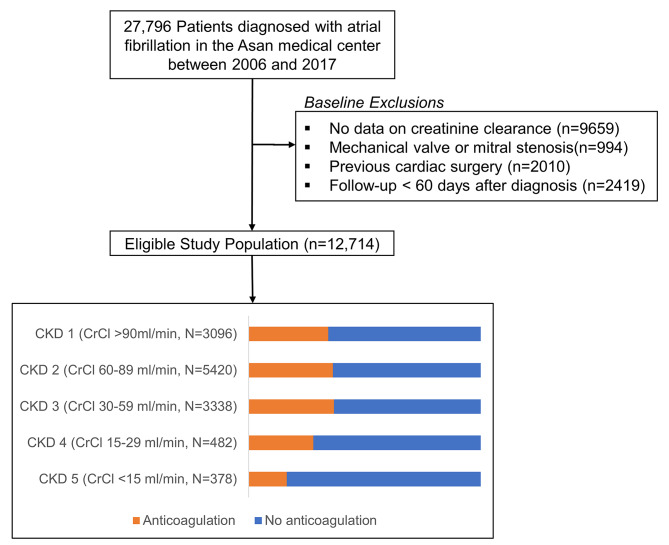
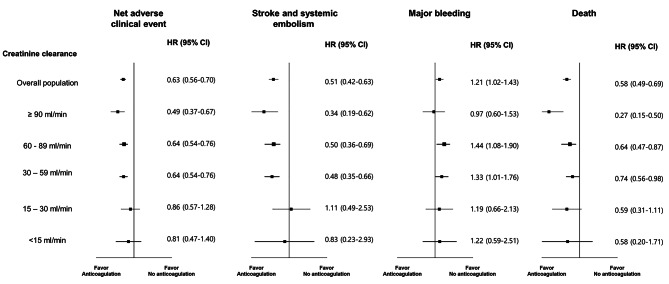
This is a retrospective observational review of patients with AF who were managed at Asan Medical Center (Seoul, Korea) between January 1, 2006, and December 31, 2018. Patients were categorized into groups according to their baseline CrCl by Cockcroft-Gault equation and their outcomes were evaluated (CKD 1, ≥ 90 mL/min; CKD2, 60-89 mL/min; CKD3, 30-59 mL/min; CKD4, 15-29 mL/min; CKD 5, < 15 mL/min). The primary outcome was NACE (net adverse clinical events), defined as a composite of all-cause mortality, thromboembolic events, and major bleeding.
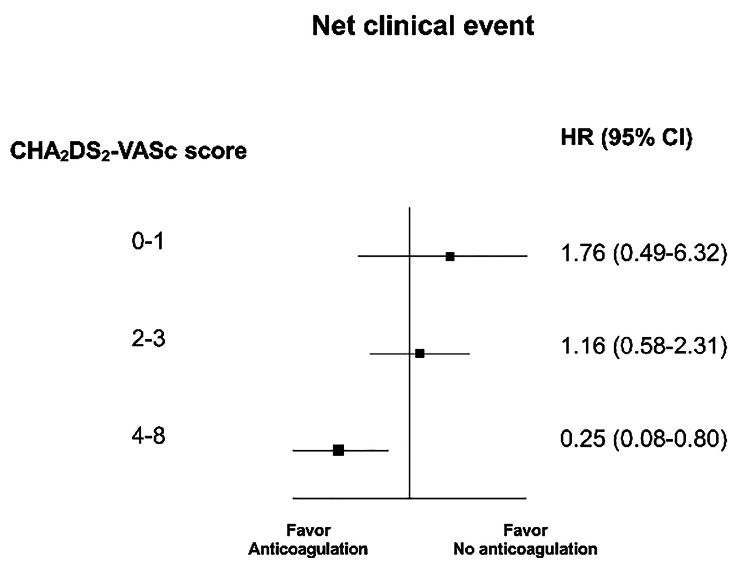
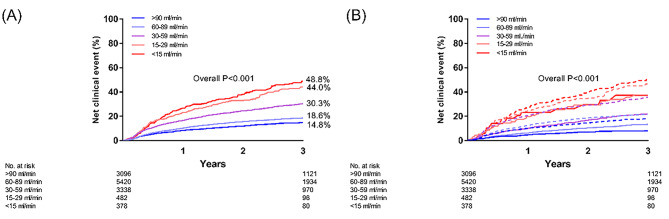
We identified 12,714 consecutive patients with AF (mean 64.6 ± 11.9 years, 65.3% male, mean CHADS-VASc score 2.4 ± 1.6 points) between 2006 and 2017. In patients receiving anticoagulation therapy (n = 4447, 35.0%), warfarin (N = 3768, 84.7%) was used more frequently than NOACs (N = 673, 15.3%). There was a higher 3-year rate of NACE with renal function deterioration (14.8%, 18.6%, 30.3%, 44.0%, and 48.8% for CKD stages 1-5, respectively).The clinical benefit of anticoagulation therapy was most prominent in patients with CKD 1 (hazard ratio [HR] 0.49, 95% confidence interval [CI] 0.37-0.67), 2 (HR 0.64 CI 0.54-0.76), and 3 (HR 0.64 CI 0.54-0.76), but not in CKD 4 (HR 0.86, CI 0.57-1.28) and 5 (HR 0.81, CI 0.47-1.40). Among patients with CKD, the benefit of anticoagulation therapy was only evident in those with a high risk of embolism (CHADS-VASc score ≥ 4, HR 0.25, CI 0.08-0.80).
Advanced CKD is associated with a higher risk of NACE. The clinical benefit of anticoagulation therapy was reduced with the increasing CKD stage.
在慢性肾脏病(CKD)患者中,抗凝治疗的临床获益和风险仍不确定。我们根据肌酐清除率(CrCl)的差异描述了接受抗凝治疗的心房颤动(AF)患者的结局。我们还旨在确定哪些患者可以从抗凝治疗中受益。
这是对 2006 年 1 月 1 日至 2018 年 12 月 31 日期间在 Asan 医疗中心(韩国首尔)接受治疗的 AF 患者进行的回顾性观察性研究。根据 Cockcroft-Gault 方程,患者按基线 CrCl 分为几组,并评估了他们的结局(CKD 1:≥90 mL/min;CKD2:60-89 mL/min;CKD3:30-59 mL/min;CKD4:15-29 mL/min;CKD 5:<15 mL/min)。主要结局是 NACE(净不良临床事件),定义为全因死亡率、血栓栓塞事件和大出血的复合结局。
我们在 2006 年至 2017 年期间确定了 12714 例连续接受 AF 治疗的患者(平均年龄 64.6±11.9 岁,65.3%为男性,平均 CHADS-VASc 评分 2.4±1.6 分)。在接受抗凝治疗的患者(n=4447,35.0%)中,华法林(n=3768,84.7%)的使用频率高于 NOAC(n=673,15.3%)。肾功能恶化时,3 年 NACE 发生率较高(CKD 1 期为 14.8%、18.6%、30.3%、44.0%和 48.8%,分别)。抗凝治疗的临床获益在 CKD 1(危险比[HR]0.49,95%置信区间[CI]0.37-0.67)、2(HR 0.64 CI 0.54-0.76)和 3(HR 0.64 CI 0.54-0.76)期患者中最为显著,但在 CKD 4(HR 0.86,CI 0.57-1.28)和 5(HR 0.81,CI 0.47-1.40)期患者中则不然。在 CKD 患者中,抗凝治疗的获益仅在栓塞风险较高的患者中(CHADS-VASc 评分≥4,HR 0.25,CI 0.08-0.80)中显现。
晚期 CKD 与 NACE 风险增加相关。抗凝治疗的临床获益随着 CKD 分期的增加而降低。