Division of Allergy and Infectious Diseases, Department of Medicine, University of Washington, Seattle.
Vaccine and Infectious Diseases Division, Fred Hutchinson Cancer Center, Seattle, Washington.
JAMA Netw Open. 2023 Apr 3;6(4):e2310039. doi: 10.1001/jamanetworkopen.2023.10039.
Development of effective, scalable therapeutics for SARS-CoV-2 is a priority.
To test the efficacy of combined tixagevimab and cilgavimab monoclonal antibodies for early COVID-19 treatment.
DESIGN, SETTING, AND PARTICIPANTS: Two phase 2 randomized blinded placebo-controlled clinical trials within the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV)-2/A5401 platform were performed at US ambulatory sites. Nonhospitalized adults 18 years or older within 10 days of positive SARS-CoV-2 test and symptom onset were eligible and were enrolled from February 1 to May 31, 2021.
Tixagevimab-cilgavimab, 300 mg (150 mg of each component) given intravenously (IV) or 600 mg (300 mg of each component) given intramuscularly (IM) in the lateral thigh, or pooled placebo.
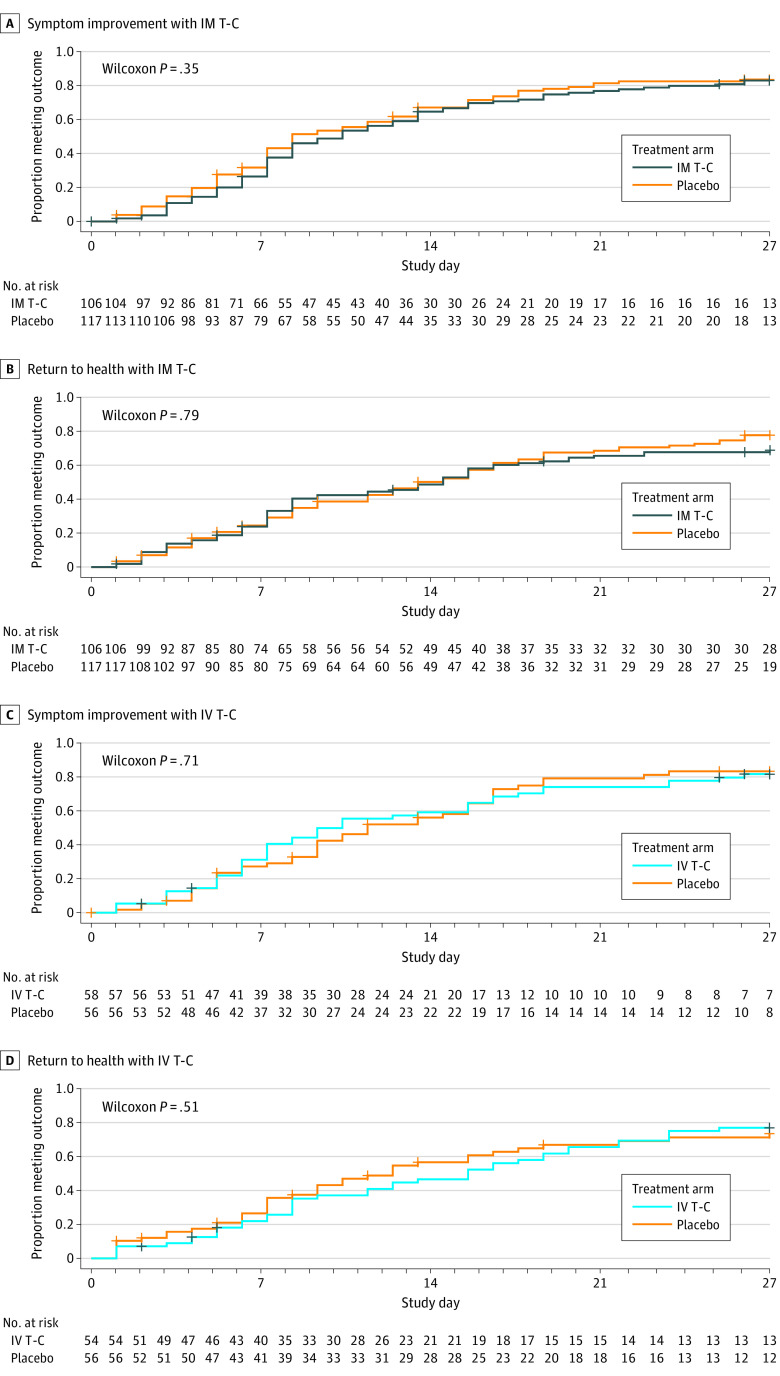
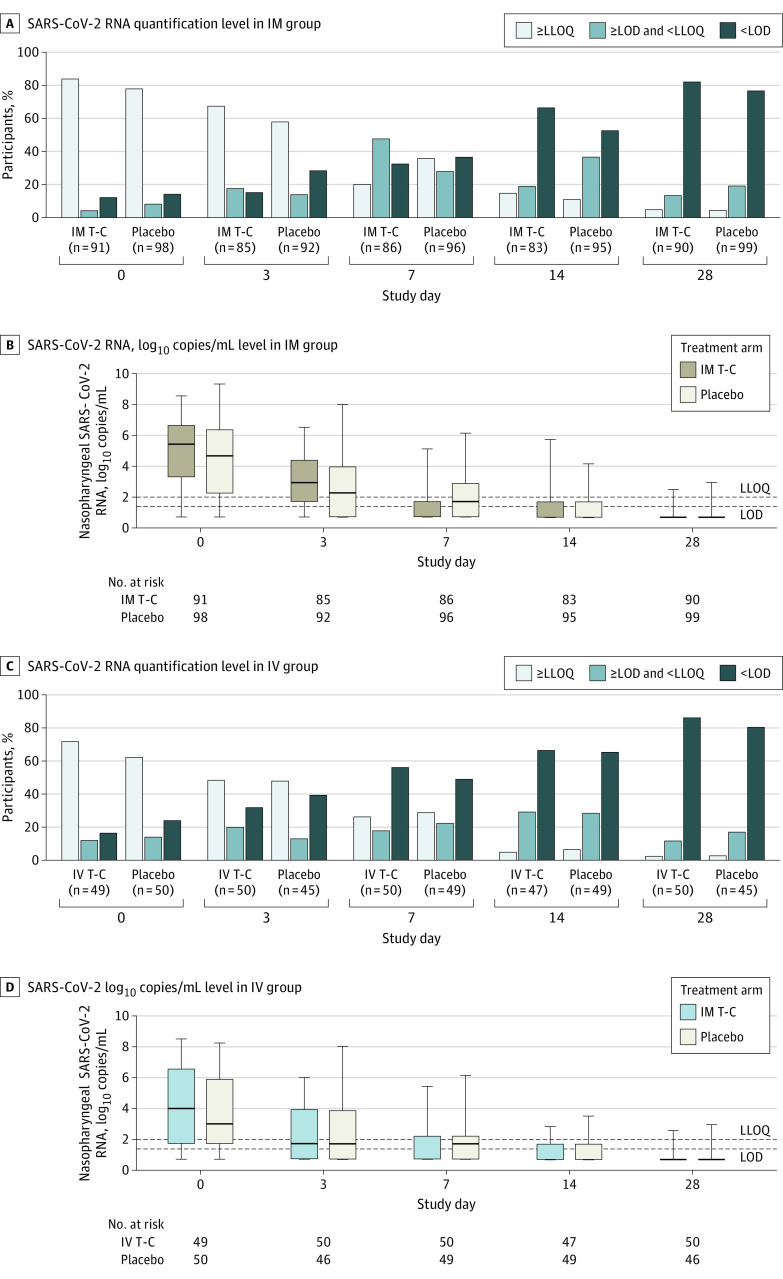
Coprimary outcomes were time to symptom improvement through 28 days; nasopharyngeal SARS-CoV-2 RNA below the lower limit of quantification (LLOQ) on days 3, 7, or 14; and treatment-emergent grade 3 or higher adverse events through 28 days.
A total of 229 participants were randomized for the IM study and 119 were randomized for the IV study. The primary modified intention-to-treat population included 223 participants who initiated IM tixagevimab-cilgavimab (n = 106) or placebo treatment (n = 117) (median age, 39 [IQR, 30-48] years; 113 [50.7%] were men) and 114 who initiated IV tixagevimab-cilgavimab (n = 58) or placebo treatment (n = 56) (median age, 44 [IQR, 35-54] years; 67 [58.8%] were women). Enrollment in the IV study was stopped early based on a decision to focus on IM product development. Participants were enrolled at a median of 6 (IQR, 4-7) days from COVID-19 symptom onset. Significant differences in time to symptom improvement were not observed for IM tixagevimab-cilgavimab vs placebo or IV tixagevimab-cilgavimab vs placebo. A greater proportion in the IM tixagevimab-cilgavimab arm (69 of 86 [80.2%]) than placebo (62 of 96 [64.6%]) had nasopharyngeal SARS-CoV-2 RNA below LLOQ at day 7 (adjusted risk ratio, 1.33 [95% CI, 1.12-1.57]) but not days 3 and 14; the joint test across time points favored treatment (P = .003). Differences in the proportion below LLOQ were not observed for IV tixagevimab-cilgavimab vs placebo at any of the specified time points. There were no safety signals with either administration route.
In these 2 phase 2 randomized clinical trials, IM or IV tixagevimab-cilgavimab was safe but did not change time to symptom improvement. Antiviral activity was more evident in the larger IM trial.
ClinicalTrials.gov Identifier: NCT04518410.
开发针对 SARS-CoV-2 的有效、可扩展的疗法是当务之急。
测试联合使用替沙格韦单抗和西加韦单抗单克隆抗体进行早期 COVID-19 治疗的疗效。
设计、地点和参与者:在美国门诊点进行了两项 2 期随机、双盲、安慰剂对照的临床试验,属于加速 COVID-19 治疗干预和疫苗(ACTIV)-2/A5401 平台。符合条件的是在 SARS-CoV-2 检测呈阳性且出现症状 10 天内的非住院成年患者,年龄在 18 岁或以上,从 2021 年 2 月 1 日至 5 月 31 日入组。
替沙格韦单抗-西加韦单抗,静脉注射(IV)给予 300mg(每组分 150mg)或肌肉注射(IM)给予 600mg(每组分 300mg),于大腿外侧,或给予混合安慰剂。
主要终点是通过 28 天症状改善的时间;第 3、7 或 14 天鼻咽 SARS-CoV-2 RNA 低于定量下限(LLOQ);以及通过 28 天出现的治疗相关 3 级或更高级别的不良事件。
共有 229 名参与者被随机分配到 IM 研究,119 名参与者被随机分配到 IV 研究。主要改良意向治疗人群包括 223 名开始接受 IM 替沙格韦单抗-西加韦单抗(n=106)或安慰剂治疗(n=117)的参与者(中位年龄 39 [IQR,30-48] 岁;113 [50.7%] 为男性)和 114 名开始接受 IV 替沙格韦单抗-西加韦单抗(n=58)或安慰剂治疗(n=56)的参与者(中位年龄 44 [IQR,35-54] 岁;67 [58.8%] 为女性)。由于决定专注于 IM 产品开发,IV 研究提前停止入组。参与者从 COVID-19 症状出现到入组的中位数时间为 6 天(IQR,4-7)。与安慰剂相比,IM 替沙格韦单抗-西加韦单抗组(86 例中的 69 例 [80.2%])与安慰剂组(96 例中的 62 例 [64.6%])在第 7 天出现症状改善的时间没有显著差异(调整后的风险比,1.33 [95% CI,1.12-1.57]),但在第 3 和第 14 天没有差异;联合各时间点的检验结果支持治疗(P=0.003)。在任何指定时间点,与安慰剂相比,IV 替沙格韦单抗-西加韦单抗组的鼻咽 SARS-CoV-2 RNA 低于 LLOQ 的比例没有差异。两种给药途径均未出现安全信号。
在这两项 2 期随机临床试验中,IM 或 IV 替沙格韦单抗-西加韦单抗是安全的,但并未改变症状改善的时间。抗病毒活性在更大的 IM 试验中更为明显。
ClinicalTrials.gov 标识符:NCT04518410。