Yan Wen-Tao, Li Chao, Yao Lan-Qing, Qiu Hai-Bo, Wang Ming-Da, Xu Xin-Fei, Zhou Ya-Hao, Wang Hong, Chen Ting-Hao, Gu Wei-Min, Zhong Jian-Hong, Wu Han, Pawlik Timothy M, Lau Wan Yee, Shen Feng, Yang Tian
Department of Hepatobiliary Surgery, Eastern Hepatobiliary Surgery Hospital, Second Military Medical University (Navy Medical University), Shanghai, China.
Graduate School, Second Military Medical University (Navy Medical University), Shanghai, China.
Hepatobiliary Surg Nutr. 2023 Apr 10;12(2):155-168. doi: 10.21037/hbsn-21-288. Epub 2021 Oct 21.
Recurrence is common among patients undergoing hepatic resection for hepatocellular carcinoma (HCC), which greatly limits long-term survival. We aimed to identify predictors and long-term prognosis of early and late recurrence after HCC resection.
Multicenter data of patients who underwent HCC resection between 2002 and 2016 were analyzed. Recurrence was divided into early (≤2 years) and late recurrence (>2 years after surgery). Predictors of early and late recurrence, and prognostic factors of post-recurrence survival (PRS) were identified by univariate and multivariate analyses.
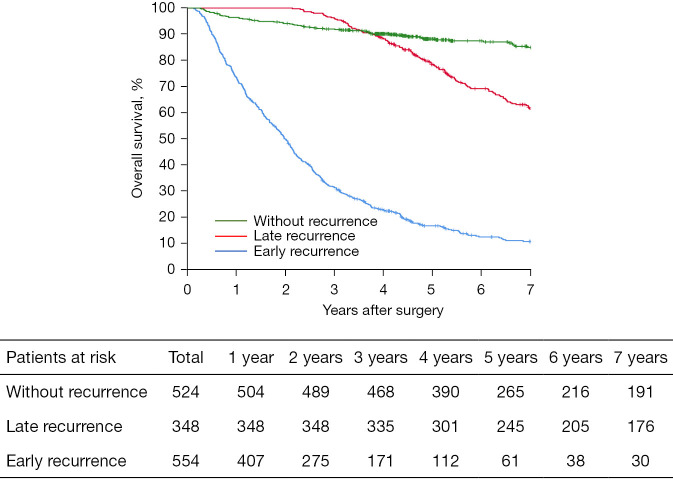
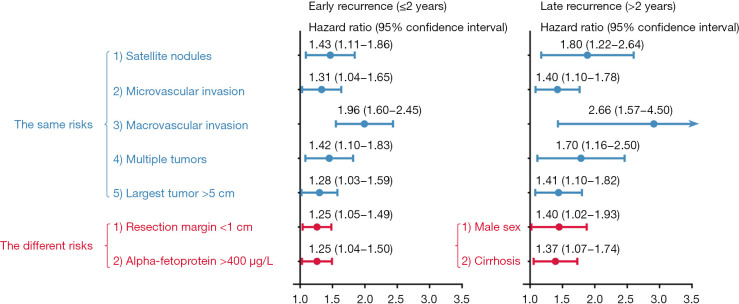
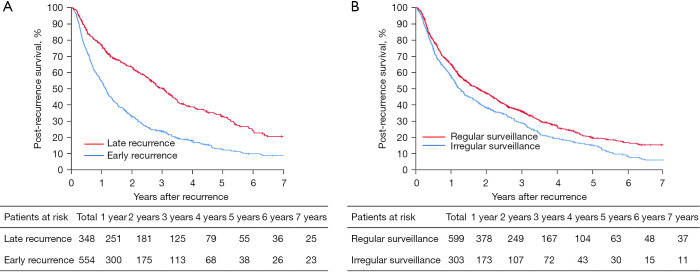
Among 1,426 patients, 554 (38.8%) and 348 (24.4%) developed early and late recurrence, respectively. Independent predictors associated with early recurrence included preoperative alpha-fetoprotein level >400 µg/L, resection margin <1 cm, and tumor size >5.0 cm, multiplicity, macrovascular and microvascular invasion, and satellites of the initial tumor at the first diagnosis of HCC; independent predictors associated with late recurrence included male, cirrhosis, and tumor size >5.0 cm, multiplicity, macrovascular and microvascular invasion, and satellites of the initial tumor. Patients with early recurrence had a lower likelihood of undergoing potentially curative treatments for recurrence (37.2% 48.0%, P<0.001) and a worse median PRS (13.5 36.6 months, P<0.001) patients who had late recurrence. Multivariate analysis revealed that early recurrence and irregular postoperative surveillance were independently associated with worse PRS [hazard ratio (HR) =1.250, 95% CI: 1.016-1.538, P=0.035; and HR =1.983, 95% CI: 1.677-2.345, P<0.001].
Predictors associated with early and late recurrence after curative resection for patients with HCC were generally same, although several did differ. Patients with late recurrence had better long-term survival than patients with early recurrence.
肝细胞癌(HCC)肝切除术后复发常见,这极大地限制了长期生存。我们旨在确定HCC切除术后早期和晚期复发的预测因素及长期预后。
分析2002年至2016年间接受HCC切除患者的多中心数据。复发分为早期(≤2年)和晚期复发(术后>2年)。通过单因素和多因素分析确定早期和晚期复发的预测因素以及复发后生存(PRS)的预后因素。
1426例患者中,分别有554例(38.8%)和348例(24.4%)发生早期和晚期复发。与早期复发相关的独立预测因素包括术前甲胎蛋白水平>400μg/L、切缘<1cm、肿瘤大小>5.0cm、肿瘤多发、大血管和微血管侵犯以及首次诊断HCC时初始肿瘤的卫星灶;与晚期复发相关的独立预测因素包括男性、肝硬化、肿瘤大小>5.0cm、肿瘤多发、大血管和微血管侵犯以及初始肿瘤的卫星灶。早期复发患者接受复发潜在根治性治疗的可能性较低(37.2%对48.0%,P<0.001),且PRS的中位生存期较差(13.5对36.6个月,P<0.001),晚期复发患者则相反。多因素分析显示,早期复发和术后不规则监测与较差的PRS独立相关[风险比(HR)=1.250,95%置信区间:1.016 - 1.538,P = 0.035;HR = 1.983,95%置信区间:1.677 - 2.345,P<0.001]。
HCC根治性切除术后早期和晚期复发的预测因素总体相同,尽管有一些确实不同。晚期复发患者的长期生存优于早期复发患者。