Peter F. Lyu (
Michael E. Chernew, Harvard University, Boston, Massachusetts.
Health Aff (Millwood). 2023 May;42(5):622-631. doi: 10.1377/hlthaff.2022.01061.
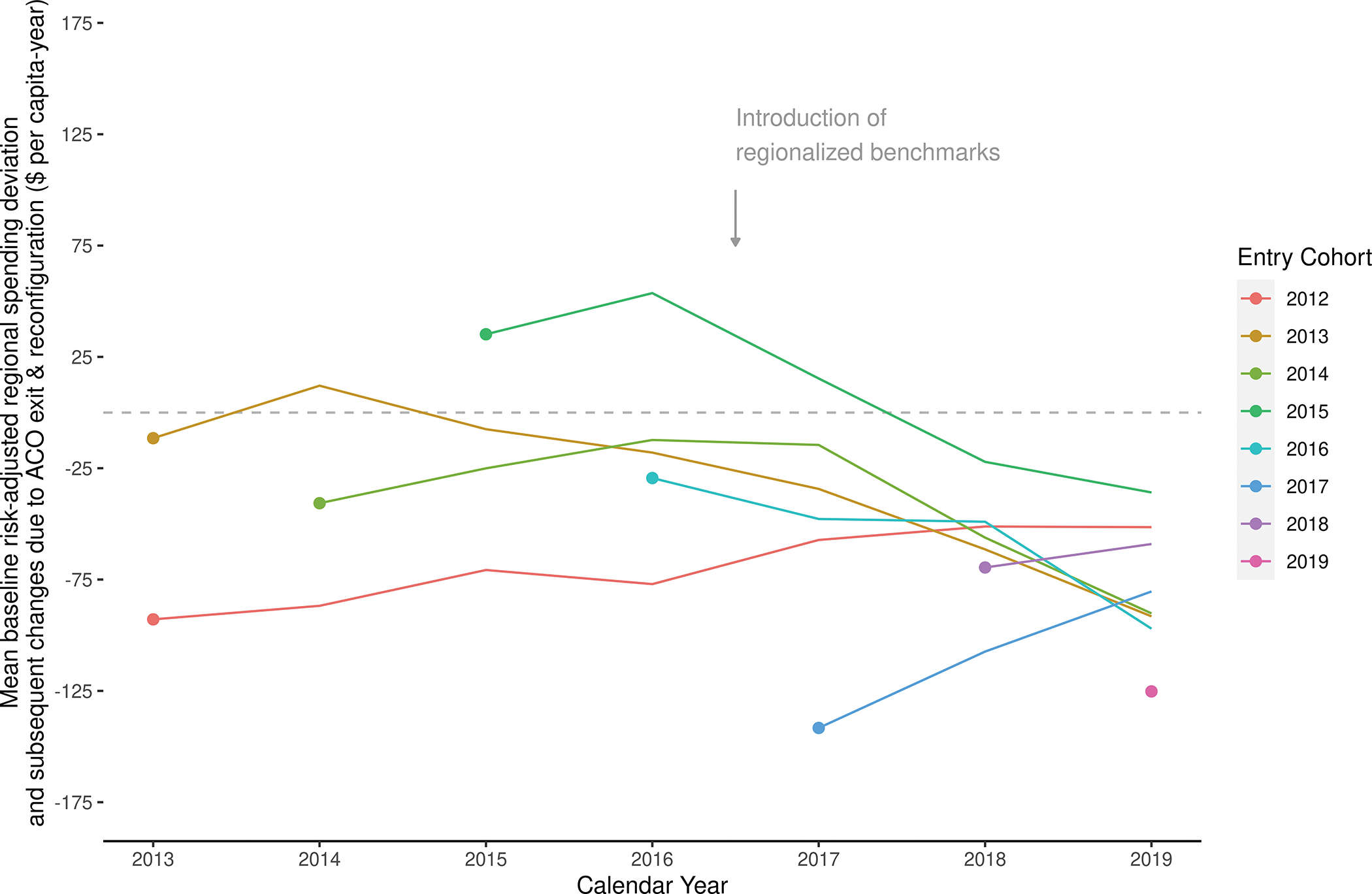
In 2017 the Medicare Shared Savings Program (MSSP) began incorporating regional spending into accountable care organization (ACO) benchmarks, thus favoring the participation of ACOs and practices with lower baseline spending than their region. To characterize providers' responses to these incentives, we isolated changes in spending due to changes in the mix of ACOs and practices participating in the MSSP. In contrast to earlier participation patterns, the composition of the MSSP after 2017 increasingly shifted to providers with lower preexisting levels of spending relative to their region, consistent with a selection response. Changes occurred through the entry of new ACOs with lower baseline spending, the exit of higher-spending ACOs, and the reconfiguration of participant lists favoring lower-spending practices within continuing ACOs. These participation patterns varied meaningfully by ACO type. Although compositional changes could not be definitively tied to benchmarking changes, the disproportionate participation of providers with lower baseline spending implies substantial costs and the need for ACO benchmarking reforms.
2017 年,医疗保险共享储蓄计划(MSSP)开始将区域支出纳入问责制医疗组织(ACO)的基准,从而有利于参与率较低的 ACO 和实践。为了描述提供者对这些激励措施的反应,我们将由于参与 MSSP 的 ACO 和实践的组合变化而导致的支出变化隔离出来。与早期的参与模式相比,2017 年后 MSSP 的组成越来越倾向于与地区相比支出较低的提供者,这与选择反应一致。变化是通过具有较低基线支出的新 ACO 的进入、较高支出的 ACO 的退出以及有利于持续 ACO 内较低支出实践的参与者名单的重新配置来实现的。这些参与模式因 ACO 类型而有很大的不同。尽管不能将构成变化明确归因于基准变化,但具有较低基线支出的提供者的不成比例参与意味着存在大量成本,需要对 ACO 基准进行改革。