From the Division of Thoracic and Upper Gastrointestinal Surgery, Department of Surgery, McGill University Health Centre, Montreal, Que. (Kammili, Cools-Lartique, Ferri); the Division of Surgical Oncology, Department of Surgery, McGill University Health Centre, Montreal, Que. (Morency); and the Division of General Surgery, Department of Surgery, McGill University Health Centre, Montreal, Que. (Mueller)
From the Division of Thoracic and Upper Gastrointestinal Surgery, Department of Surgery, McGill University Health Centre, Montreal, Que. (Kammili, Cools-Lartique, Ferri); the Division of Surgical Oncology, Department of Surgery, McGill University Health Centre, Montreal, Que. (Morency); and the Division of General Surgery, Department of Surgery, McGill University Health Centre, Montreal, Que. (Mueller).
Can J Surg. 2023 May 2;66(3):E219-E227. doi: 10.1503/cjs.019420. Print 2023 May-Jun.
Patients living in rural communities experience difficulty accessing specialized medical care. Rural patients with cancer present with more advanced disease, have reduced access to treatment and have poorer overall survival than urban patients. This study's aim was to evaluate outcomes of patients with gastric cancer living in rural and remote areas versus urban and suburban communities in the context of an established care corridor to a tertiary care centre.
All patients treated for gastric cancer at the McGill University Health Centre during 2010-2018 were included. Travel, lodging and cancer care coordination were provided for patients from remote and rural areas and coordinated centrally by dedicated nurse navigators servicing these regions. Statistics Canada's remoteness index was used to categorize patients into a rural and remote group and an urban and suburban group.
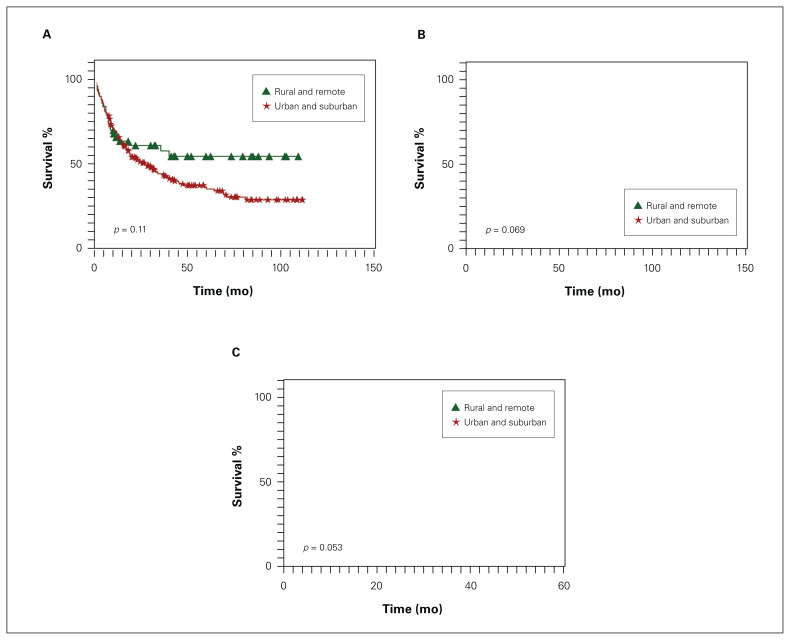
A total of 274 patients were included. Compared with patients from urban and suburban areas, patients from rural and remote areas were younger and their clinical tumour stage was higher at presentation. The number of curative resections and palliative surgeries and rate of nonresection were comparable ( = 0.96). Overall, disease-free and progression-free survival were comparable between the groups, and having locally advanced cancer correlated with poorer survival ( < 0.001).
Although patients with gastric cancer from rural and remote areas had more advanced disease at presentation, their treatment patterns and survival were comparable to those of patients from urbanized areas in the context of a publicly funded care corridor to a multidisciplinary specialist cancer centre. Equitable access to health care is necessary to diminish any preexisting disparities among patients with gastric cancer.
农村社区的患者在获得专业医疗方面存在困难。患有癌症的农村患者疾病更为晚期,获得治疗的机会减少,整体生存率低于城市患者。本研究旨在评估在为农村和偏远地区患者建立通往三级治疗中心的既定护理通道的背景下,农村和偏远地区与城市和郊区社区的胃癌患者的治疗效果。
纳入 2010 年至 2018 年在麦吉尔大学健康中心接受治疗的所有胃癌患者。为来自偏远和农村地区的患者提供交通、住宿和癌症护理协调,并由专门的护士导航员提供服务,由中央协调这些地区的服务。使用加拿大统计局的偏远指数将患者分为农村和偏远地区组以及城市和郊区组。
共纳入 274 名患者。与来自城市和郊区地区的患者相比,来自农村和偏远地区的患者年龄更小,就诊时临床肿瘤分期更高。根治性切除和姑息性手术的数量以及非切除率相当(=0.96)。总体而言,两组患者的无病生存和无进展生存相当,局部晚期癌症与较差的生存相关(<0.001)。
尽管农村和偏远地区的胃癌患者就诊时疾病更为晚期,但在为多学科专家癌症中心提供公共资助的护理通道的背景下,他们的治疗模式和生存情况与城市地区的患者相当。为胃癌患者提供公平的医疗保健服务是必要的,以减少任何现有的患者之间的差异。