Um Samnang, Vang Daraden, Pin Punleak, Chau Darapheak
National Institute of Public Health (NIPH), Phnom Penh, Cambodia.
Doctoral specialization in Pneumology, Faculty of Medicine at the University of Health Sciences (UHS) in Phnom Penh, Phnom Penh, Cambodia.
PLOS Glob Public Health. 2023 May 3;3(5):e0001440. doi: 10.1371/journal.pgph.0001440. eCollection 2023.
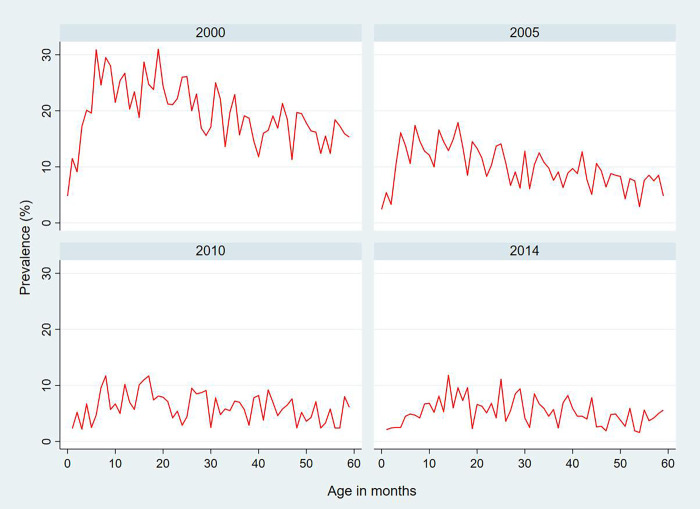
Acute Respiratory Infections (ARIs) are the leading cause of mortality and morbidity among children under 5 years old and about 1.3 million annually worldwide. Account for 33% of deaths among children under 5 years that occurred in developing countries. In Cambodia, ARIs prevalence in children under 5 years old was 20% in 2000, and 6% in 2014. Hence, the aimed to describe the trends of ARI symptoms among children aged 0-59 months over time using the 2000, 2005, 2010, and 2014 Cambodia Demographic and Health Survey (CDHS) and determined the relationships between socio-demographic, behavioral, and environmental factors with ARI symptoms. We analyzed existing children's data from 2000, 2005, 2010 and 2014 of Cambodia Demographic and Health Survey (CDHS) that used a two-stage stratified cluster sampling design. We limited our analysis to children born in the last five years prior to the surveys, alive and living in households during interview time. Data were pooled across the four survey years for 29,171 children aged 0-59 months. All statistics were carried out using STATA V16, and survey weights were taken into account for the survey design of the CDHS. We used multiple logistic regression to determine the main predictors of ARI symptoms among children under 5 years. ARI symptoms in the previous two weeks in children aged 0-59 months in Cambodia were 19.9% in 2000 to 8.6% in 2005 to 6.4% in 2010, and 5.5% in 2014. Factors independently associated with increased odds of ARI symptoms were children ages 6-11 months with adjusted odds ratio [AOR = 1.91; 95% CI: 1.53-2.38], 12-23 months [AOR = 1.79; 95% CI: 1.46-2.20], and 24-35 months [AOR = 1.41; 95% CI: 1.13-1.76], smoking mother [AOR = 1.61; 95% CI: 1.27-2.05], and using non-improved toilets in households [AOR = 1.20; 95% CI: 0.99-1.46]. However, the following factors were found to be associated with decreased odds of having ARI symptoms: Mothers with higher education [AOR = 0.45; 95% CI: 0.21-0.94], breastfeeding children [AOR = 0.87; 95% CI: 0.77-0.98], and children born into richest wealth quantile [AOR = 0.73; 95% CI: 0.56-0.95], respectively. Survey 2005 [AOR = 0.36; 95% CI: 0.31-0.42], 2010 [AOR = 0.27; 95% CI: 0.22-0.33], 2014 [AOR = 0.24; 95% CI: 0.19-0.30]. The trends of ARI symptoms among children under five in Cambodia significantly decreased from 2000-2014. Smoking mothers, young children ages (0-35 months), and using non-improved toilet in household are factors that independently increased the likelihood that children would develop ARI symptoms. Inversely, factors were found to be associated with decreased odds of having ARI symptoms: Mothers with higher education, breastfeeding children, and children born into the richest wealth quantile and Survey years. Therefore, government and child family programs must promote maternal education, particularly infant breastfeeding. The government ought to support maternal education and infant breastfeeding in the interest of early childhood care.
急性呼吸道感染(ARIs)是全球5岁以下儿童死亡和发病的主要原因,每年约有130万例。占发展中国家5岁以下儿童死亡人数的33%。在柬埔寨,2000年5岁以下儿童的ARI患病率为20%,2014年为6%。因此,旨在利用2000年、2005年、2010年和2014年柬埔寨人口与健康调查(CDHS)描述0至59个月儿童ARI症状随时间的变化趋势,并确定社会人口、行为和环境因素与ARI症状之间的关系。我们分析了柬埔寨人口与健康调查(CDHS)2000年、2005年、2010年和2014年现有的儿童数据,该调查采用两阶段分层整群抽样设计。我们将分析限制在调查前五年出生、在访谈时存活且居住在家庭中的儿童。对29171名0至59个月儿童的四个调查年份的数据进行了汇总。所有统计均使用STATA V16进行,并考虑了CDHS调查设计的调查权重。我们使用多元逻辑回归来确定5岁以下儿童ARI症状的主要预测因素。柬埔寨0至59个月儿童前两周的ARI症状在2000年为19.9%,2005年为8.6%,2010年为6.4%,2014年为5.5%。与ARI症状几率增加独立相关的因素是6至11个月的儿童,调整后的优势比[AOR = 1.91;95%置信区间:1.53 - 2.38],12至23个月[AOR = 1.79;95%置信区间:1.46 - 2.20],以及24至35个月[AOR = 1.41;95%置信区间:1.13 - 1.76],母亲吸烟[AOR = 1.61;95%置信区间:1.27 - 2.05],以及家庭使用未改善的厕所[AOR = 1.20;95%置信区间:0.99 - 1.46]。然而,发现以下因素与ARI症状几率降低相关:受过高等教育的母亲[AOR = 0.45;95%置信区间:0.21 - 0.94],母乳喂养的儿童[AOR = 0.87;95%置信区间:0.77 - 0.98],以及出生在最富裕财富五分位数的儿童[AOR = 0.73;95%置信区间:0.56 - 0.95],分别。2005年调查[AOR = 0.36;95%置信区间:0.31 - 0.42],2010年[AOR = 0.27;95%置信区间:0.22 - 0.33],2014年[AOR = 0.24;95%置信区间:0.19 - 0.30]。2000年至2014年,柬埔寨5岁以下儿童的ARI症状趋势显著下降。母亲吸烟、幼儿年龄(0至35个月)以及家庭使用未改善的厕所是独立增加儿童患ARI症状可能性的因素。相反,发现与ARI症状几率降低相关的因素是:受过高等教育的母亲、母乳喂养的儿童、出生在最富裕财富五分位数的儿童以及调查年份。因此,政府和儿童家庭项目必须促进孕产妇教育,特别是婴儿母乳喂养。政府应该为了幼儿护理支持孕产妇教育和婴儿母乳喂养。