Pan Heng-Chi, Chen Hsing-Yu, Chen Hui-Ming, Huang Yu-Tung, Fang Ji-Tseng, Chen Yung-Chang
Chang Gung University College of Medicine, Taoyuan, Taiwan.
Division of Nephrology, Department of Internal Medicine, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan.
Front Med (Lausanne). 2023 Apr 17;10:1153670. doi: 10.3389/fmed.2023.1153670. eCollection 2023.
Critically ill patients with acute kidney injury (AKI) have a poor prognosis. Recently, the Acute Disease Quality Initiative (ADQI) proposed to define acute kidney disease (AKD) as acute or subacute damage and/or loss of kidney function post AKI. We aimed to identify the risk factors for the occurrence of AKD and to determine the predictive value of AKD for 180-day mortality in critically ill patients.
We evaluated 11,045 AKI survivors and 5,178 AKD patients without AKI, who were admitted to the intensive care unit between 1 January 2001 and 31 May 2018, from the Chang Gung Research Database in Taiwan. The primary and secondary outcomes were the occurrence of AKD and 180-day mortality.
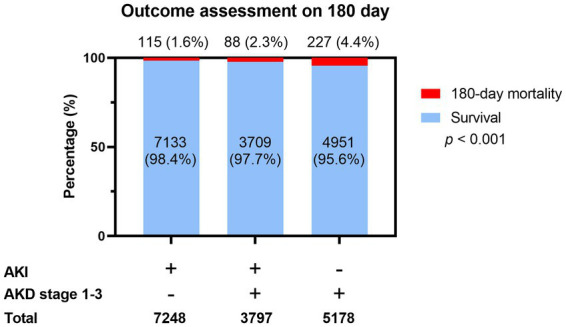
The incidence rate of AKD among AKI patients who did not receive dialysis or died within 90 days was 34.4% (3,797 of 11,045 patients). Multivariable logistic regression analysis indicated that AKI severity, underlying early CKD, chronic liver disease, malignancy, and use of emergency hemodialysis were independent risk factors of AKD, while male gender, higher lactate levels, use of ECMO, and admission to surgical ICU were negatively correlated with AKD. 180-day mortality was highest among AKD patients without AKI during hospitalization (4.4%, 227 of 5,178 patients), followed by AKI with AKD (2.3%, 88 of 3,797 patients) and AKI without AKD (1.6%, 115 of 7,133 patients). AKI with AKD had a borderline significantly increased risk of 180-day mortality (aOR 1.34, 95% CI 1.00-1.78; = 0.047), while patients with AKD but no preceding AKI episodes had the highest risk (aOR 2.25, 95% CI 1.71-2.97; < 0.001).
The occurrence of AKD adds limited additional prognostic information for risk stratification of survivors among critically ill patients with AKI but could predict prognosis in survivors without prior AKI.
急性肾损伤(AKI)的重症患者预后较差。最近,急性疾病质量改进计划(ADQI)提议将急性肾病(AKD)定义为AKI后急性或亚急性肾功能损害和/或丧失。我们旨在确定AKD发生的危险因素,并确定AKD对重症患者180天死亡率的预测价值。
我们从台湾长庚研究数据库中评估了2001年1月1日至2018年5月31日期间入住重症监护病房的11045例AKI幸存者和5178例无AKI的AKD患者。主要和次要结局分别为AKD的发生和180天死亡率。
在未接受透析或在90天内死亡的AKI患者中,AKD的发生率为34.4%(11045例患者中的3797例)。多变量逻辑回归分析表明,AKI严重程度、潜在的早期慢性肾脏病(CKD)、慢性肝病、恶性肿瘤和使用急诊血液透析是AKD的独立危险因素,而男性、较高的乳酸水平、使用体外膜肺氧合(ECMO)和入住外科重症监护病房与AKD呈负相关。住院期间无AKI的AKD患者180天死亡率最高(4.4%,5178例患者中的227例),其次是合并AKD的AKI患者(2.3%,3797例患者中的88例)和无AKD的AKI患者(1.6%,7133例患者中的115例)。合并AKD的AKI患者180天死亡风险有临界显著增加(调整后比值比[aOR]1.34,95%置信区间[CI]1.00-1.78;P=0.047),而有AKD但无前AKI发作的患者风险最高(aOR 2.25,95%CI 1.71-2.97;P<0.001)。
AKD的发生为AKI重症患者幸存者的风险分层增加的预后信息有限,但可预测无先前AKI的幸存者的预后。