Department of Endocrinology, Diabetes and Metabolism, Centro Hospitalar E Universitário de Coimbra, 3004-561, Coimbra, Portugal.
Department of Nephrology, Centro Hospitalar E Universitário de Coimbra, 3004-561, Coimbra, Portugal.
Acta Diabetol. 2023 Sep;60(9):1179-1185. doi: 10.1007/s00592-023-02112-0. Epub 2023 May 13.
Acute kidney injury (AKI) is highly prevalent during hospitalization of patients with type 2 diabetes (T2D). We aimed to assess the impact of AKI and its severity and duration on the risk of hypoglycaemia in hospitalized patients with T2D.
Retrospective cohort analysis of patients with T2D, admitted at a University Hospital in 2018-2019. AKI was defined as an increase in serum creatinine by ≥ 0.3 mg/dl (48 h) or ≥ 1.5 times baseline (7 days), and hypoglycaemia as blood glucose concentration < 70 mg/dl. Patients with chronic kidney disease stage ≥ 4 were excluded. We registered 239 hospitalizations with AKI and randomly selected 239 without AKI (control). Multiple logistic regression was used to adjust for confounding factors and ROC curve analysis to determine a cutoff for AKI duration.
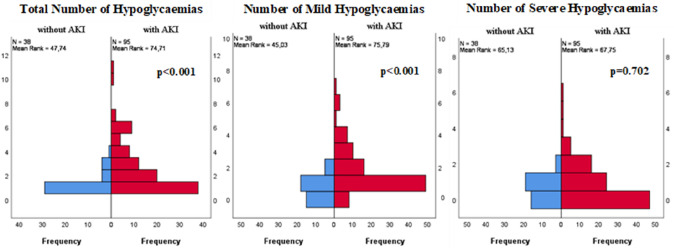
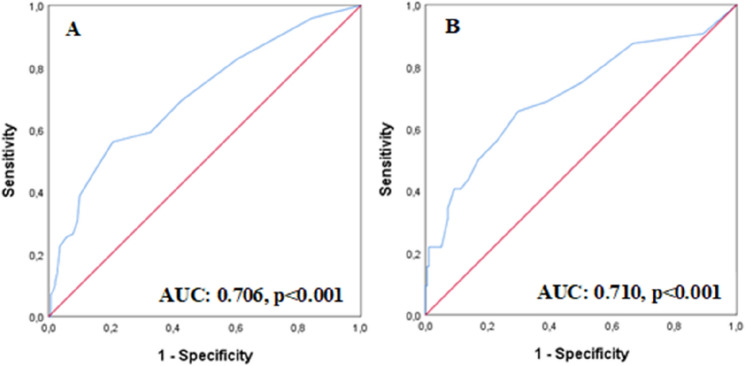
The risk of hypoglycaemia was higher in the AKI group (crude OR 3.6, 95%CI 1.8-9.6), even after adjusting for covariates (OR 4.2, 95%CI 1.8-9.6). Each day of AKI duration was associated with a 14% increase in the risk of hypoglycaemia (95%CI 1.1-1.2), and a cutoff of 5.5 days of AKI duration was obtained for increased risk of hypoglycaemia and mortality. AKI severity was also associated with mortality, but showed no significant association with hypoglycaemia. Patients with hypoglycaemia had 4.4 times greater risk of mortality (95%CI 2.4-8.2).
AKI increased the risk of hypoglycaemia during hospitalization of patients with T2D, and its duration was the main risk factor. These results highlight the need for specific protocols to avoid hypoglycaemia and its burden in patients with AKI.
急性肾损伤(AKI)在 2 型糖尿病(T2D)患者住院期间高发。本研究旨在评估 AKI 及其严重程度和持续时间对 T2D 住院患者发生低血糖的风险的影响。
回顾性分析了 2018 年至 2019 年在一所大学医院住院的 T2D 患者。AKI 的定义为血清肌酐升高≥0.3mg/dl(48 小时)或≥基础值的 1.5 倍(7 天),低血糖定义为血糖浓度<70mg/dl。排除慢性肾脏病 4 期及以上患者。共登记了 239 例 AKI 住院患者和 239 例无 AKI(对照组)住院患者。采用多因素逻辑回归调整混杂因素,并进行 ROC 曲线分析确定 AKI 持续时间的截断值。
AKI 组发生低血糖的风险更高(粗 OR 3.6,95%CI 1.8-9.6),即使在调整了混杂因素后也是如此(OR 4.2,95%CI 1.8-9.6)。AKI 持续时间每增加一天,发生低血糖的风险增加 14%(95%CI 1.1-1.2),AKI 持续时间为 5.5 天时,低血糖和死亡的风险增加。AKI 严重程度也与死亡率相关,但与低血糖无显著关联。发生低血糖的患者死亡风险增加 4.4 倍(95%CI 2.4-8.2)。
AKI 增加了 T2D 患者住院期间发生低血糖的风险,其持续时间是主要的危险因素。这些结果强调了需要制定特定的方案来避免 AKI 患者发生低血糖及其带来的负担。