Vlachopoulou Dimitra, Balomenakis Charalampos, Kartas Anastasios, Samaras Athanasios, Papazoglou Andreas S, Moysidis Dimitrios V, Barmpagiannos Konstantinos, Kyriakou Melina, Papanastasiou Anastasios, Baroutidou Amalia, Vouloagkas Ioannis, Tzikas Apostolos, Giannakoulas George
First Department of Cardiology, AHEPA University Hospital, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, 546 36 Thessaloniki, Greece.
Interbalkan European Medical Center, Asklipiou 10, 555 35 Thessaloniki, Greece.
J Clin Med. 2023 Apr 23;12(9):3063. doi: 10.3390/jcm12093063.
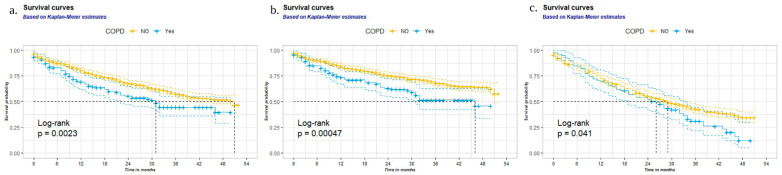
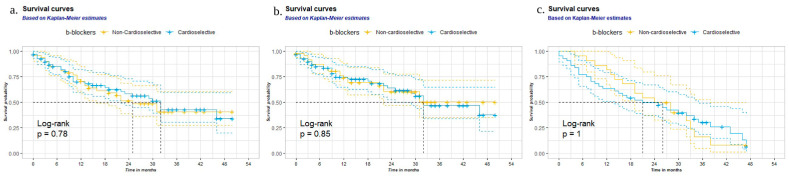
Atrial fibrillation (AF) and chronic obstructive pulmonary disease (COPD) have been independently associated with increased mortality; however, there is no evidence regarding beta-blocker cardioselectivity and long-term outcomes in patients with AF and concurrent COPD. This post hoc analysis of the MISOAC-AF randomized trial (NCT02941978) included patients hospitalized with comorbid AF. At discharge, all patients were classified according to the presence of COPD; patients with COPD on beta-blockers were classified according to beta-blocker cardioselectivity. Adjusted hazard ratios (aHRs) were calculated by using multivariable Cox regression models. The primary outcome was all-cause mortality, and the secondary outcomes were cardiovascular mortality and hospitalizations. Of 1103 patients with AF, 145 (13%) had comorbid COPD. Comorbid COPD was associated with an increased risk of all-cause (aHR, 1.33; 95% confidence interval (CI), 1.02 to 1.73) and cardiovascular mortality (aHR 1.47; 95% CI, 1.10 to 1.99), but not with increased risk of hospitalizations (aHR 1.10; 95% CI, 0.82 to 1.48). The use of cardioselective versus non-cardioselective beta-blockers was associated with similar all-cause mortality (aHR 1.10; 95% CI, 0.63 to 1.94), cardiovascular mortality (aHR 1.33; 95% CI, 0.71 to 2.51), and hospitalizations (aHR 1.65; 95% CI 0.80 to 3.38). In recently hospitalized patients with AF, the presence of COPD was independently associated with increased risk of all-cause and cardiovascular mortality. No difference between cardioselective and non-cardioselective beta-blockers, regarding clinical outcomes, was identified.
心房颤动(AF)和慢性阻塞性肺疾病(COPD)均与死亡率增加独立相关;然而,尚无证据表明β受体阻滞剂的心脏选择性与合并AF和COPD患者的长期预后有关。这项对MISOAC-AF随机试验(NCT02941978)的事后分析纳入了因合并AF住院的患者。出院时,所有患者根据是否患有COPD进行分类;使用β受体阻滞剂的COPD患者根据β受体阻滞剂的心脏选择性进行分类。采用多变量Cox回归模型计算调整后的风险比(aHR)。主要结局为全因死亡率,次要结局为心血管死亡率和住院率。在1103例AF患者中,145例(13%)合并COPD。合并COPD与全因死亡风险增加(aHR,1.33;95%置信区间(CI),1.02至1.73)和心血管死亡率增加(aHR 1.47;95%CI,1.10至1.99)相关,但与住院风险增加无关(aHR 1.10;95%CI,0.82至1.48)。使用心脏选择性β受体阻滞剂与非心脏选择性β受体阻滞剂的全因死亡率(aHR 1.10;95%CI,0.63至1.94)、心血管死亡率(aHR 1.33;95%CI,0.71至2.51)和住院率(aHR 1.65;95%CI 0.80至3.38)相似。在近期因AF住院的患者中,COPD的存在与全因和心血管死亡风险增加独立相关。未发现心脏选择性和非心脏选择性β受体阻滞剂在临床结局方面存在差异。