Rao Jingade Krishnojirao Dayashankara
Dept of Maxillo Facial Surgery & Diagnostic Science College of Dentistry, Qassim University, Saudi Arabia.
J Oral Biol Craniofac Res. 2023 May-Jun;13(3):424-428. doi: 10.1016/j.jobcr.2023.04.001. Epub 2023 Apr 28.
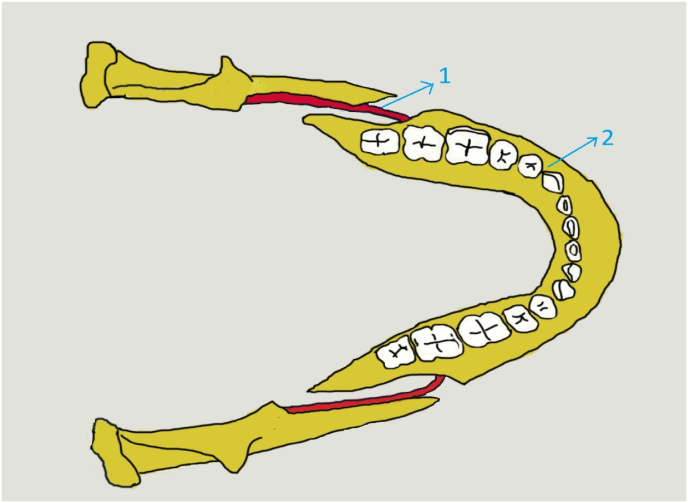
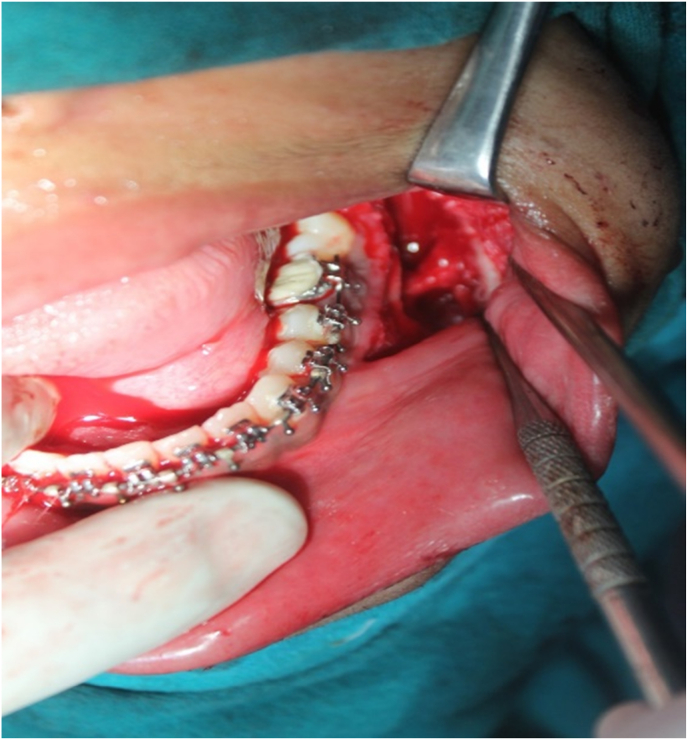
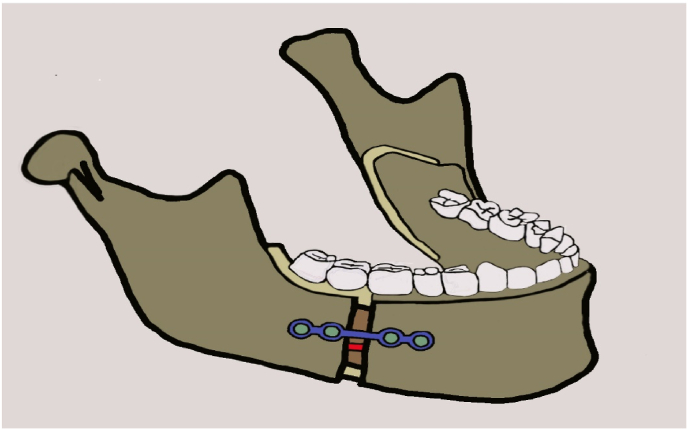
Inferior alveolar nerve (IAN) injury is most common in bilateral sagittal split osteotomy (BSSO) cases. The present standard is to always reposition the IAN from the proximal fragment to the distal fragment during surgery. This study aims to assess the severity and incidence of postoperative injury and the recovery of the inferior alveolar nerve in proximal fragment entrapment.
There was no significant difference between the groups in the recovery of IAN sensation after 6 months and the 1-year period. Hence reposition of IAN from the proximal segment to the distal segment during BSSO surgery may not be mandatory if the required movement is within 6 mm. This avoids unnecessary manipulation of the IAN over the proximal fragment.
下牙槽神经(IAN)损伤在双侧矢状劈开截骨术(BSSO)病例中最为常见。目前的标准是在手术过程中始终将IAN从近端骨块重新定位到远端骨块。本研究旨在评估术后损伤的严重程度和发生率以及近端骨块嵌顿情况下下牙槽神经的恢复情况。
共选择35例(70例BSSO截骨术)下颌畸形需要移动等于或小于6毫米的患者。70例截骨术中,有20例在劈开时IAN位于近端骨块(第1组)。第2组包括同一患者中IAN位于远端骨段的20例截骨术。因此,本研究排除了15例双侧IAN位于远端骨段的患者。所有BSSO手术均由同一位外科医生进行。术后恢复情况和随访在术后第1天以及3个月、6个月和12个月时进行。由一位对手术不知情的第三位临床医生进行痛觉(针刺辨别)测试和用棉纤维进行的机械感受性触觉皮肤测试,以评估IAN感觉。
6个月和1年期间两组IAN感觉恢复情况无显著差异。因此,如果所需移动在6毫米以内,BSSO手术期间将IAN从近端骨段重新定位到远端骨段可能不是必需的。这避免了对近端骨块上IAN的不必要操作。