Department of Cancer Imaging, Peter MacCallum Cancer Centre, Melbourne, Australia.
The Sir Peter MacCallum Department of Oncology, The University of Melbourne, Melbourne, Australia.
Eur J Nucl Med Mol Imaging. 2023 Aug;50(10):2997-3010. doi: 10.1007/s00259-023-06257-6. Epub 2023 May 15.
Peptide Receptor Radionuclide Therapy (PRRT) delivers targeted radiation to Somatostatin Receptor (SSR) expressing Neuroendocrine Neoplasms (NEN). We sought to assess the predictive and prognostic implications of tumour dosimetry with respect to response by Ga DOTATATE (GaTate) PET/CT molecular imaging tumour volume of SSR (MITV) change and RECIST 1.1, and overall survival (OS).
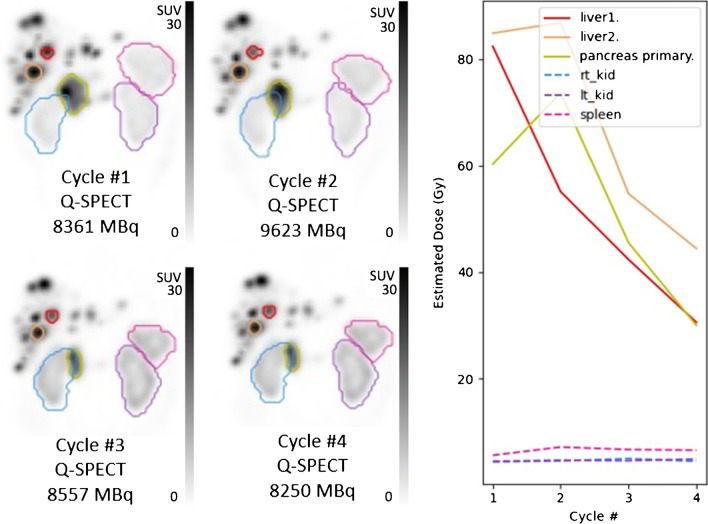
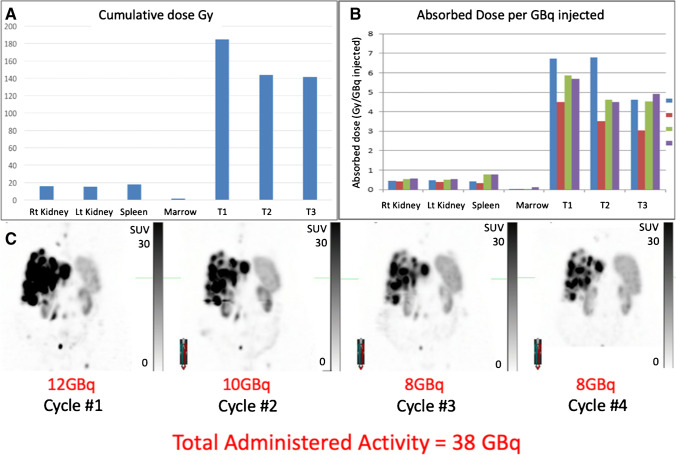
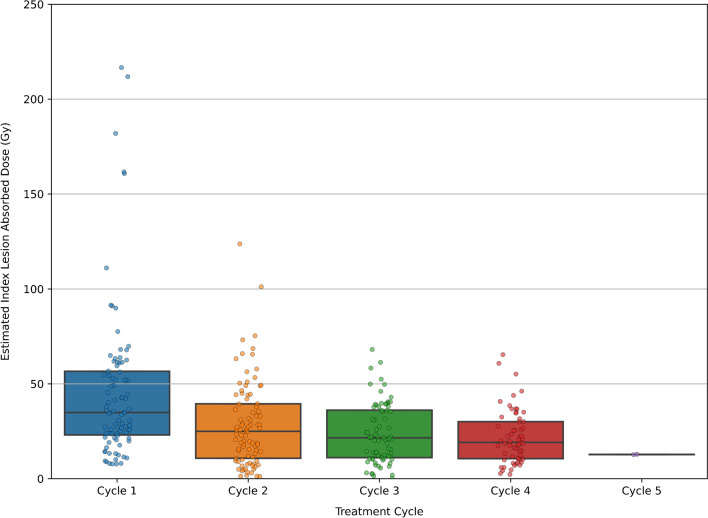
Patients with gastro-entero-pancreatic (GEP) NEN who received LuTate followed by quantitative SPECT/CT (Q-SPECT/CT) the next day (Jul 2010 to Jan 2019) were retrospectively reviewed. Single time-point (STP) lesional dosimetry was performed for each cycle using population-based pharmacokinetic modelling. MITV and RECIST 1.1 were measured at 3-months post PRRT.
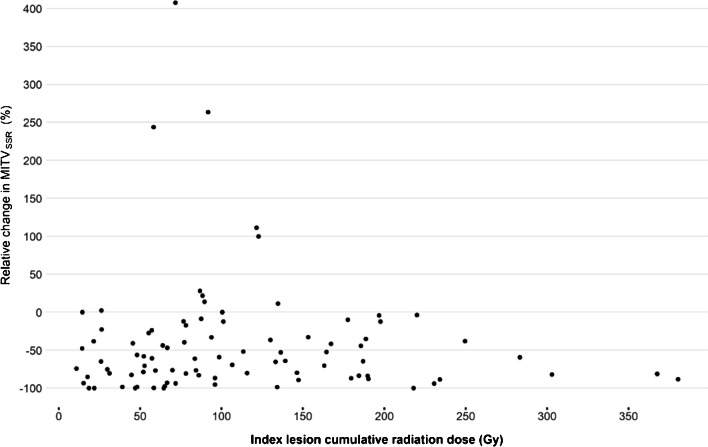
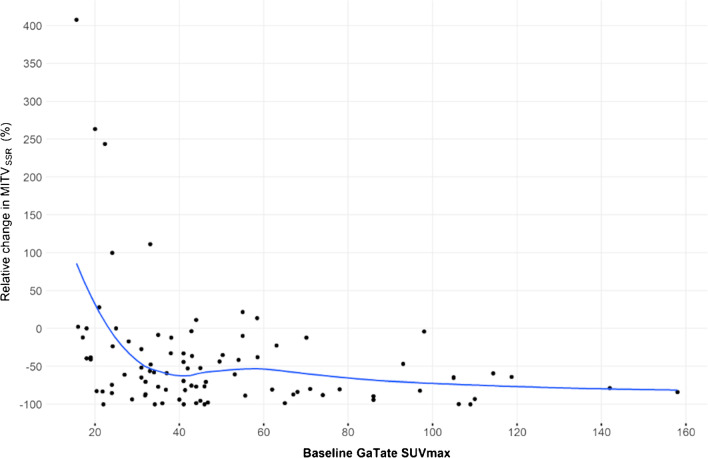
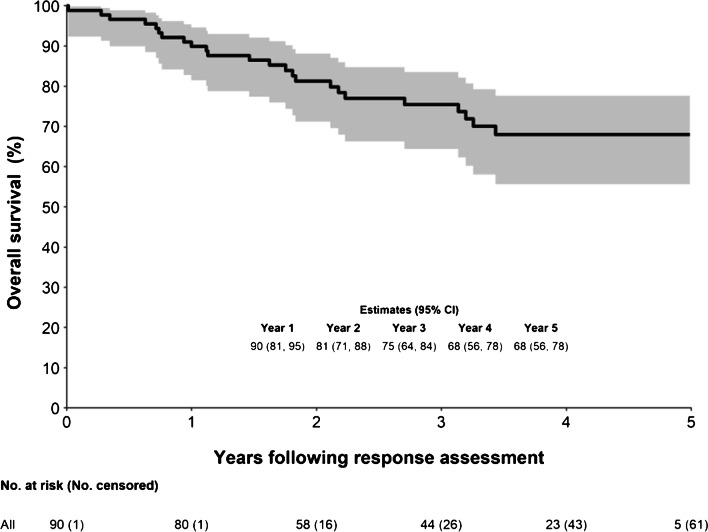
Median of 4 PRRT cycles were administered to 90 patients (range 2-5 cycles; mean 27.4 GBq cumulative activity; mean 7.6 GBq per cycle). 68% received at least one cycle with radiosensitising chemotherapy (RSC). RECIST 1.1 partial response was 24%, with 70% stable and 7% progressive disease. Cycle 1 radiation dose in measurable lesions was associated with local response (odds ratio 1.5 per 50 Gy [95% CI: 1.1-2.0], p = 0.002) when adjusted by tumour grade and RSC. Median change in MITV was -63% (interquartile range -84 to -29), with no correlation with radiation dose to the most avid lesion on univariable or multivariant analyses (5.6 per 10 Gy [95% CI: -1.6, 12.8], p = 0.133). OS at 5-years was 68% (95% CI: 56-78%). Neither baseline MITV (hazard ratio 1.1 [95% CI: 1.0, 1.2], p = 0.128) nor change in baseline MITV (hazard ratio 1.0 [95% CI: 1.0, 1.1], p = 0.223) were associated with OS when adjusted by tumour grade and RSC but RSC was (95% CI: 0.2, 0.8, p = 0.012).
Radiation dose to tumour during PRRT was predictive of radiologic response but not survival. Survival outcomes may relate to other biological factors. There was no evidence that MITV change was associated with OS, but a larger study is needed.
评估肽受体放射性核素治疗 (PRRT) 中肿瘤剂量学对 18F-DOTATATE (GaTate) PET/CT 分子成像中生长抑素受体 (SSR) 表达神经内分泌肿瘤 (NEN) 肿瘤体积变化和 RECIST 1.1 以及总生存期 (OS) 反应的预测和预后意义。
回顾性分析了 2010 年 7 月至 2019 年 1 月期间接受 LuTate 治疗并在第二天进行定量 SPECT/CT (Q-SPECT/CT) 的胃肠胰神经内分泌肿瘤 (GEP) NEN 患者。使用基于人群的药代动力学模型对每个周期进行单次时间点 (STP) 病变剂量测定。PRRT 后 3 个月测量 MITV 和 RECIST 1.1。
90 例患者接受了中位数为 4 个周期的 PRRT(范围 2-5 个周期;平均累积活动 27.4GBq;平均每个周期 7.6GBq)。68%的患者至少接受了一次放射增敏化疗 (RSC)。RECIST 1.1 的部分缓解率为 24%,稳定率为 70%,进展率为 7%。当调整肿瘤分级和 RSC 后,可测量病变的第 1 周期辐射剂量与局部反应相关(每 50Gy 的优势比为 1.5[95%CI:1.1-2.0],p=0.002)。MITV 的中位数变化为-63%(四分位距-84 至-29),单变量和多变量分析均未发现与最活跃病变的辐射剂量相关(每 10Gy 增加 5.6[95%CI:-1.6,12.8],p=0.133)。5 年 OS 为 68%(95%CI:56-78%)。调整肿瘤分级和 RSC 后,基线 MITV(风险比 1.1[95%CI:1.0,1.2],p=0.128)或基线 MITV 变化(风险比 1.0[95%CI:1.0,1.1],p=0.223)均与 OS 无关,但 RSC 相关(95%CI:0.2,0.8,p=0.012)。
PRRT 期间肿瘤的辐射剂量与影像学反应相关,但与生存无关。生存结果可能与其他生物学因素有关。没有证据表明 MITV 变化与 OS 相关,但需要更大的研究。