Division of Thoracic Surgery, Sichuan Cancer Research Center for Cancer, Sichuan Cancer Hospital and Institute, Sichuan Cancer Center, Afliated Cancer Hospital of University of Electronic Science and Technology of China, Chengdu, Sichuan, People's Republic of China.
Int J Surg. 2023 Jul 1;109(7):2001-2009. doi: 10.1097/JS9.0000000000000436.
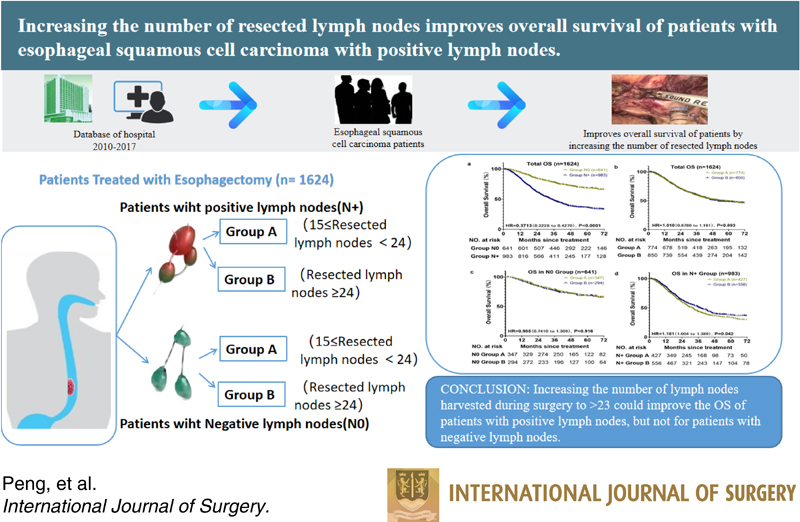
The incidence and mortality of esophageal cancer are high. Therefore, the authors aimed to investigate how the number of dissected lymph nodes (LNs) during esophagectomy for esophageal squamous cell carcinoma impacts overall survival (OS), particularly that of patients with positive LNs.
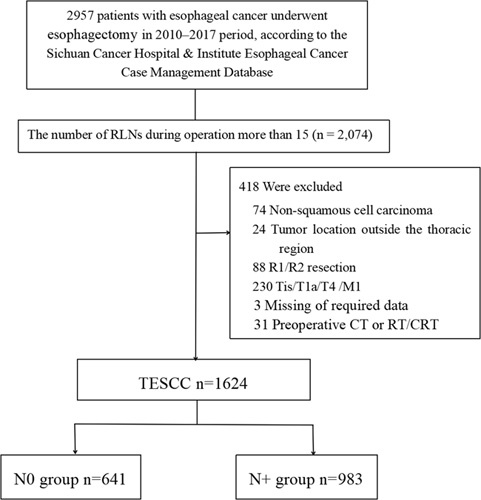
Data from 2010 to 2017 were obtained from the Sichuan Cancer Hospital and Institute Esophageal Cancer Case Management Database. Participants were divided into two groups: patients with negative lymph nodes (N0) and patients with positive lymph nodes (N+). The median number of resected LNs during surgery was 24; therefore, patients with 15-23 and those with 24 or more resected LNs were assigned to subgroups A and B, respectively.
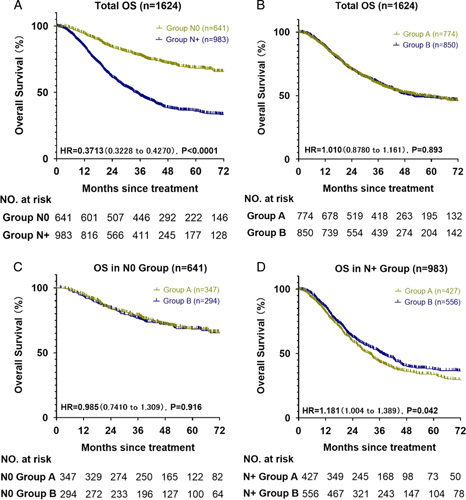
After a median follow-up of 60.33 months, 1624 patients who underwent esophagectomy were evaluated; 60.53 and 39.47% had a pathological diagnosis of N+ or N0, respectively. The median OS was 33.9 months for the N+ group; however, the N0 group did not achieve the median OS. The mean OS was 84.9 months. In the N+ group, the median OS times of subgroups A and B were 31.2 and 37.1 months, respectively. The OS rates at 1, 3, and 5 years were 82, 43, and 34%, respectively, for subgroup A of the N+ group; they were 86, 51, and 38%, respectively, for subgroup B of the N+ group. Subgroups A and B of the N0 group exhibited no statistically significant differences.
Increasing the number of LNs harvested during surgery to 24 or more could improve the OS of patients with positive LNs but not that of patients with negative LNs.
食管癌的发病率和死亡率都很高。因此,作者旨在研究食管癌根治术中清扫的淋巴结(LNs)数量对总生存(OS)的影响,尤其是对阳性淋巴结(LNs)患者的影响。
本研究的数据来自 2010 年至 2017 年四川省癌症医院和研究所食管癌病例管理数据库。参与者被分为两组:阴性淋巴结(N0)患者和阳性淋巴结(N+)患者。手术中切除的淋巴结中位数为 24 个;因此,15-23 个和 24 个或更多个切除淋巴结的患者分别被分配到亚组 A 和 B。
在中位随访 60.33 个月后,对 1624 例行食管癌切除术的患者进行了评估;病理诊断为 N+和 N0 的患者分别占 60.53%和 39.47%。N+组的中位 OS 为 33.9 个月;然而,N0 组未达到中位 OS。平均 OS 为 84.9 个月。在 N+组中,亚组 A 和 B 的中位 OS 时间分别为 31.2 和 37.1 个月。N+组亚组 A 的 1、3 和 5 年 OS 率分别为 82%、43%和 34%;N+组亚组 B 的 1、3 和 5 年 OS 率分别为 86%、51%和 38%。N0 组的亚组 A 和 B 之间无统计学显著差异。
增加手术中淋巴结的清扫数量至 24 个或更多可以提高阳性淋巴结患者的 OS,但不能提高阴性淋巴结患者的 OS。