Department of Internal Medicine I, Division of Endocrinology and Diabetes, University Hospital, University of Würzburg, Würzburg, Germany.
Department of Dermatology and Allergology, University Hospital Augsburg, Augsburg, Germany.
Front Endocrinol (Lausanne). 2023 May 8;14:1123132. doi: 10.3389/fendo.2023.1123132. eCollection 2023.
Adrenal incidentalomas with cortisol autonomy are associated with increased cardiovascular morbidity and mortality. Specific data on the clinical and biochemical course of affected patients are lacking.
Retrospective study from a tertiary referral centre in Germany. After exclusion of overt hormone excess, malignancy and glucocorticoid medication, patients with adrenal incidentalomas were stratified according to serum cortisol after 1 mg dexamethasone: autonomous cortisol secretion (ACS), >5.0; possible ACS (PACS), 1.9-5.0; non-functioning adenomas (NFA), ≤1.8 µg/dl.
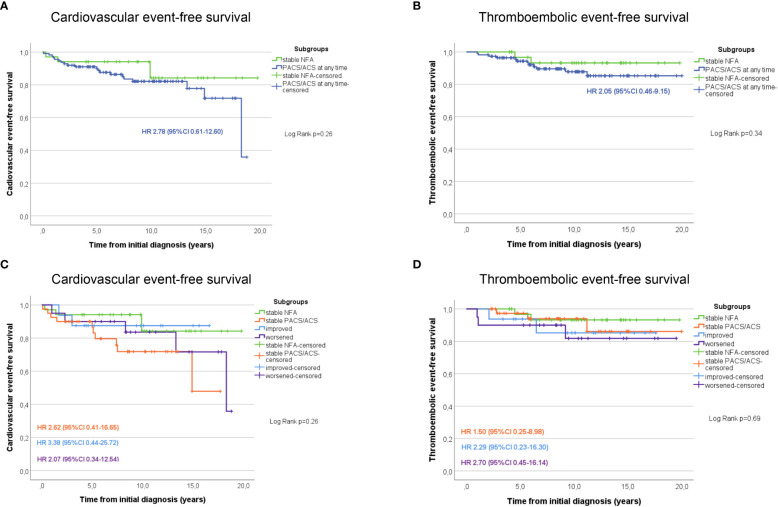
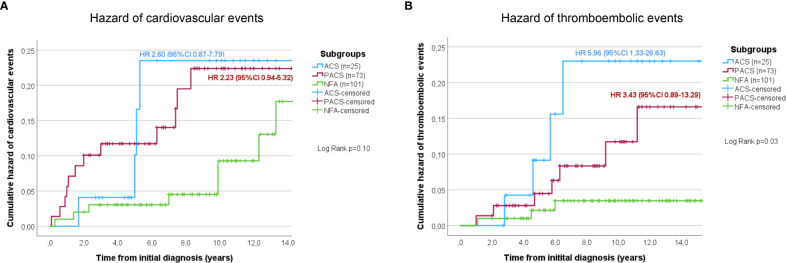
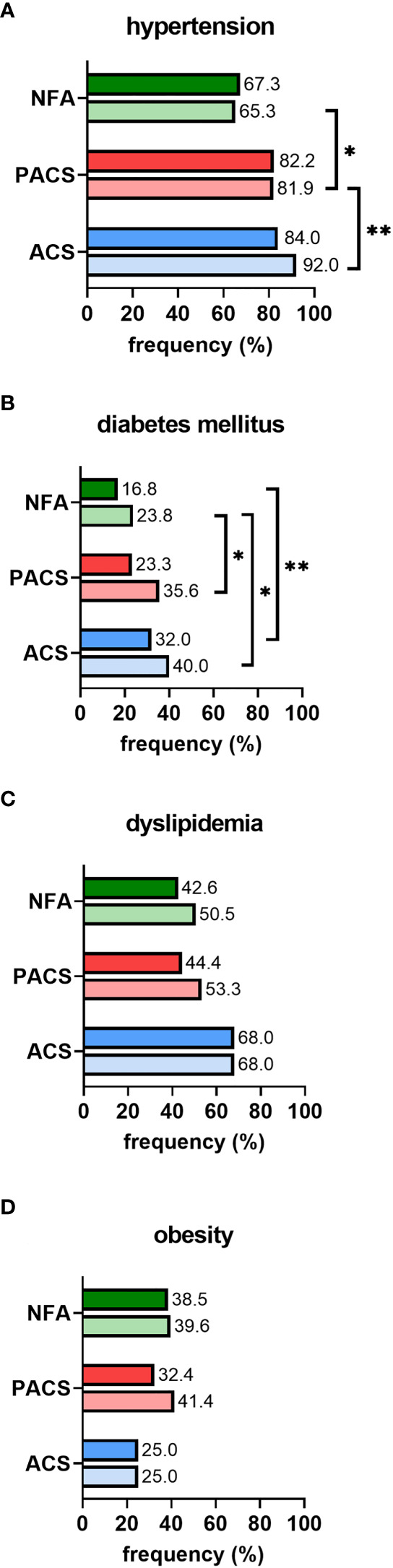
A total of 260 patients were enrolled (147 women (56.5%), median follow-up 8.8 (2.0-20.8) years). At initial diagnosis, median age was 59.5 (20-82) years, and median tumour size was 27 (10-116) mm. Bilateral tumours were more prevalent in ACS (30.0%) and PACS (21.9%) than in NFA (8.1%). Over time, 40/124 (32.3%) patients had a shift of their hormonal secretion pattern (NFA to PACS/ACS, n=15/53; PACS to ACS, n=6/47; ACS to PACS, n=11/24; PACS to NFA, n=8/47). However, none of the patients developed overt Cushing's syndrome. Sixty-one patients underwent adrenalectomy (NFA, 17.9%; PACS, 24.0%; ACS, 39.0%). When non-operated patients with NFA were compared to PACS and ACS at last follow-up, arterial hypertension (65.3% vs. 81.9% and 92.0%; p<0.05), diabetes (23.8% vs. 35.6% and 40.0%; p<0.01), and thromboembolic events (PACS: HR 3.43, 95%-CI 0.89-13.29; ACS: HR 5.96, 95%-CI 1.33-26.63; p<0.05) were significantly less frequent, along with a trend towards a higher rate of cardiovascular events in case of cortisol autonomy (PACS: HR 2.23, 95%-CI 0.94-5.32; ACS: HR 2.60, 95%-CI 0.87-7.79; p=0.1). Twenty-five (12.6%) of the non-operated patients died, with higher overall mortality in PACS (HR 2.6, 95%-CI 1.0-4.7; p=0.083) and ACS (HR 4.7, 95%-CI 1.6-13.3; p<0.005) compared to NFA. In operated patients, prevalence of arterial hypertension decreased significantly (77.0% at diagnosis to 61.7% at last follow-up; p<0.05). The prevalence of cardiovascular events and mortality did not differ significantly between operated and non-operated patients, whereas thromboembolic events were significantly less frequent in the surgical treatment group.
Our study confirms relevant cardiovascular morbidity in patients with adrenal incidentalomas (especially those with cortisol autonomy). These patients should therefore be monitored carefully, including adequate treatment of typical cardiovascular risk factors. Adrenalectomy was associated with a significantly decreased prevalence of hypertension. However, more than 30% of patients required reclassification according to repeated dexamethasone suppression tests. Thus, cortisol autonomy should ideally be confirmed before making any relevant treatment decision (e.g. adrenalectomy).
具有皮质醇自主性的肾上腺意外瘤与心血管发病率和死亡率增加有关。关于受影响患者的临床和生化病程的具体数据尚不清楚。
这是一项来自德国一家三级转诊中心的回顾性研究。在排除明显的激素过多、恶性肿瘤和糖皮质激素药物治疗后,根据 1 毫克地塞米松后血清皮质醇将肾上腺意外瘤患者分层:皮质醇自主性分泌(ACS),>5.0;可能的 ACS(PACS),1.9-5.0;无功能腺瘤(NFA),≤1.8µg/dl。
共纳入 260 例患者(女性 147 例(56.5%),中位随访时间 8.8(2.0-20.8)年)。在初始诊断时,中位年龄为 59.5(20-82)岁,肿瘤大小中位数为 27(10-116)mm。ACS(30.0%)和 PACS(21.9%)中双侧肿瘤比 NFA(8.1%)更常见。随着时间的推移,40/124 例(32.3%)患者的激素分泌模式发生了变化(NFA 转为 PACS/ACS,15/53 例;PACS 转为 ACS,6/47 例;ACS 转为 PACS,11/24 例;PACS 转为 NFA,8/47 例)。然而,没有患者出现明显的库欣综合征。61 例患者接受了肾上腺切除术(NFA,17.9%;PACS,24.0%;ACS,39.0%)。在最后一次随访时,与未手术的 NFA 患者相比,PACS 和 ACS 患者的动脉高血压(65.3% vs. 81.9%和 92.0%;p<0.05)、糖尿病(23.8% vs. 35.6%和 40.0%;p<0.01)和血栓栓塞事件(PACS:HR 3.43,95%-CI 0.89-13.29;ACS:HR 5.96,95%-CI 1.33-26.63;p<0.05)明显减少,而皮质醇自主性的心血管事件发生率呈上升趋势(PACS:HR 2.23,95%-CI 0.94-5.32;ACS:HR 2.60,95%-CI 0.87-7.79;p=0.1)。25 例(12.6%)未手术患者死亡,PACS(HR 2.6,95%-CI 1.0-4.7;p=0.083)和 ACS(HR 4.7,95%-CI 1.6-13.3;p<0.005)的总体死亡率高于 NFA。在手术患者中,动脉高血压的患病率显著下降(从诊断时的 77.0%降至最后一次随访时的 61.7%;p<0.05)。手术和未手术患者的心血管事件和死亡率无显著差异,而手术治疗组血栓栓塞事件明显减少。
我们的研究证实了肾上腺意外瘤患者存在明显的心血管发病率(尤其是皮质醇自主性患者)。因此,这些患者应接受仔细监测,包括对典型心血管危险因素的充分治疗。肾上腺切除术与高血压患病率显著降低相关。然而,超过 30%的患者需要根据重复地塞米松抑制试验进行重新分类。因此,皮质醇自主性理想情况下应在做出任何相关治疗决策之前(例如肾上腺切除术)得到确认。