Hochberg Uri, Ingelmo Pablo, Solé Ester, Miró Jordi, Rivera Gonzalo, Perez Jordi
Pain Institute of the Tel Aviv Sourasky Medical Center, Tel Aviv, Israel.
Alan Edwards Centre for Research on Pain, McGill University, Montreal, Quebec, Canada.
J Pain Res. 2023 May 18;16:1663-1671. doi: 10.2147/JPR.S405808. eCollection 2023.
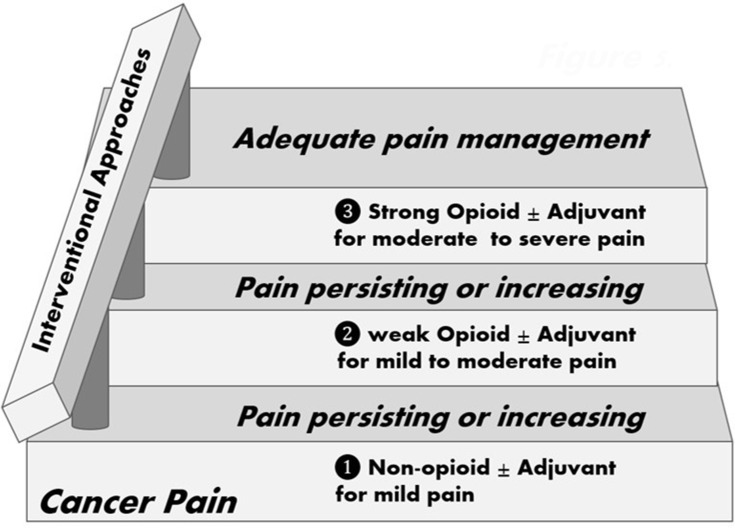
Between 10% and 20% of patients with cancer-related pain cannot achieve adequate control following the three-step ladder guidelines by the World Health Organization. Therefore, a "fourth step", including interventional approaches, has been suggested for those cases. Systematic reviews support the early use of interventional procedures to treat refractory cancer pain, control symptoms and prevent opioid dose escalation. There is strong evidence of the efficacy of celiac plexus or splanchnic neurolysis, vertebroplasty, kyphoplasty and intrathecal drug delivery. Those procedures have been found to be associated with a decrease in the symptom burden and opioid consumption, improved quality of life, and suggested as having a potentially positive impact on survival. Several studies have recommended using specific interventional techniques at earlier stages, possibly even when opioid treatment is first being considered. Conversely, leaving these options as a last analgesic resource might not be advisable since the burden these procedures might impose on too ill patients is significant. The objective of this review was to collect the available evidence published on the use of interventional treatments for refractory cancer pain with a particular interest in comparing early versus late indications. The results of the search demonstrated a very low number and quality of articles particularly addressing this question. This scarce number of evidence precluded performing a systematic analysis. A detailed and narrative description of the potential benefits of integrating interventional techniques into clinical guidelines at the early stages of the disease is provided.
在患有癌症相关疼痛的患者中,10%至20%的患者按照世界卫生组织的三阶梯指南无法实现充分控制。因此,对于这些病例,有人建议采取包括介入治疗方法在内的“第四步”。系统评价支持早期使用介入程序来治疗难治性癌症疼痛、控制症状并防止阿片类药物剂量增加。有强有力的证据表明腹腔神经丛或内脏神经松解术、椎体成形术、后凸成形术和鞘内药物递送的有效性。已发现这些程序与症状负担减轻和阿片类药物消耗减少、生活质量改善相关,并且被认为对生存可能有积极影响。几项研究建议在更早阶段使用特定的介入技术,甚至可能在首次考虑阿片类药物治疗时就使用。相反,将这些选择留作最后的镇痛资源可能并不可取,因为这些程序可能给病情过重的患者带来的负担很大。本综述的目的是收集已发表的关于使用介入治疗难治性癌症疼痛的现有证据,特别关注比较早期与晚期适应症。检索结果显示专门针对这个问题的文章数量和质量都非常低。证据数量稀少,无法进行系统分析。本文提供了关于在疾病早期将介入技术纳入临床指南的潜在益处的详细叙述性描述。