4th Department of Internal Medicine, National and Kapodistrian University of Athens School of Medicine, Attikon University General Hospital, Chaidari, Greece.
Clinical Microbiology Laboratory, National and Kapodistrian University of Athens School of Medicine, Attikon University General Hospital, Chaidari, Greece.
Rheumatology (Oxford). 2024 Feb 1;63(2):534-541. doi: 10.1093/rheumatology/kead236.
B-cell depleting monoclonal antibodies are associated with increased COVID-19 severity and impaired immune response to vaccination. We aimed to assess the humoral and cell mediated (CMI) immune response after SARS-CoV-2 vaccination in rituximab (RTX)-treated rheumatic patients.
Serum and whole blood samples were collected from RTX-treated rheumatic patients 3-6 months after last vaccination against SARS-CoV-2. Serum was tested by ELISA for quantitative detection of anti-spike SARS-CoV-2 IgG. Cell-mediated variant-specific SARS-CoV-2 immunity (CMI) was assessed by interferon-γ release assay Covi-FERON FIA. Patients were interviewed for breakthrough COVID-19 infection (BTI) 3 months post sampling.
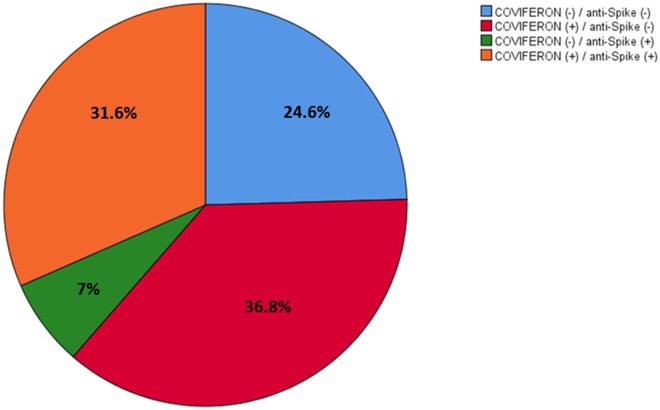
Sixty patients were studied after a median (IQR) of 179 (117-221.5) days from last vaccine to sampling. Forty (66.7%) patients had positive Covi-FERON and 23 (38.3%) had detectable anti-spike IgG. Covi-FERON positive patients had lower median RTX cumulative dose [6 (4-10.75) vs 11 (6.75-14.75) grams, (P = 0.019)]. Patients with positive anti-spike IgG had received fewer RTX cycles [2 (2-4) vs 6 (4-8), P = 0.002] and cumulative dose [4 (3-7) vs 10 (6.25-13) grams, P = 0.002] and had shorter time from last vaccination to sampling [140 (76-199) vs 192 (128-230) days, P = 0.047]. Thirty-seven percent were positive only for Covi-FERON and 7% only for anti-spike IgG. Twenty (33.3%) BTI occurred post sampling, exclusively during Omicron variant predominance. The proportion of patients with CMI response against Delta variant was lower in patients who experienced BTI (25% vs 55%, P = 0.03).
Four out of ten RTX-treated vaccinated patients show lasting cell-mediated immune response despite undetectable anti-spike antibodies. Cumulative RTX dose affects both humoral and cell-mediated responses to SARS-CoV-2 vaccines. Cell-mediated immune responses call for attention as a vaccine efficacy marker against SARS-CoV-2.
B 细胞耗竭单克隆抗体与 COVID-19 严重程度增加和疫苗接种后免疫应答受损有关。我们旨在评估利妥昔单抗(RTX)治疗的风湿性疾病患者接种 SARS-CoV-2 疫苗后的体液和细胞介导(CMI)免疫反应。
在接种 SARS-CoV-2 疫苗后 3-6 个月,从 RTX 治疗的风湿性疾病患者中采集血清和全血样本。通过 ELISA 定量检测抗刺突 SARS-CoV-2 IgG 来检测血清。通过干扰素-γ释放试验 Covi-FERON FIA 评估细胞介导的变异特异性 SARS-CoV-2 免疫(CMI)。在采样后 3 个月对患者进行突破性 COVID-19 感染(BTI)的访谈。
在最后一次疫苗接种到采样的中位数(IQR)179(117-221.5)天后,对 60 名患者进行了研究。40 名(66.7%)患者的 Covi-FERON 阳性,23 名(38.3%)患者可检测到抗刺突 IgG。Covi-FERON 阳性患者的 RTX 累积剂量中位数较低[6(4-10.75)与 11(6.75-14.75)克,(P=0.019)]。抗刺突 IgG 阳性患者接受的 RTX 周期[2(2-4)与 6(4-8),(P=0.002)]和累积剂量[4(3-7)与 10(6.25-13)克,(P=0.002)]较少,最后一次疫苗接种到采样的时间[140(76-199)与 192(128-230)天,(P=0.047)]较短。37%的患者仅对 Covi-FERON 阳性,7%的患者仅对抗刺突 IgG 阳性。20 名(33.3%)患者在采样后发生 BTI,仅在 Omicron 变体占主导地位期间发生。经历 BTI 的患者对 Delta 变体的细胞介导免疫反应比例较低(25%与 55%,P=0.03)。
尽管无法检测到抗刺突抗体,但十分之四的 RTX 治疗接种疫苗的患者仍显示出持久的细胞介导免疫反应。RTX 累积剂量影响 SARS-CoV-2 疫苗的体液和细胞介导反应。细胞介导的免疫反应需要引起关注,作为 SARS-CoV-2 疫苗的疗效标志物。