University of Oslo, NO-0316, Oslo, Norway.
Department of Pathology, Vestfold Hospital Trust, NO-3103, Tonsberg, Norway.
Diagn Pathol. 2023 May 27;18(1):70. doi: 10.1186/s13000-023-01357-1.
ROS1 fusion is an infrequent, but attractive target for therapy in patients with metastatic non- small-cell lung cancer. In studies on mainly late-stage disease, the prevalence of ROS1 fusions is about 1-3%. In early-stage lung cancer ROS1 might also provide a fruitful target for neoadjuvant or adjuvant therapy. In the present study, we investigated the prevalence of ROS1 fusion in a Norwegian cohort of early-stage lung cancer. We also explored whether positive ROS1 immunohistochemical (IHC) stain was associated with certain mutations, clinical characteristics and outcomes.
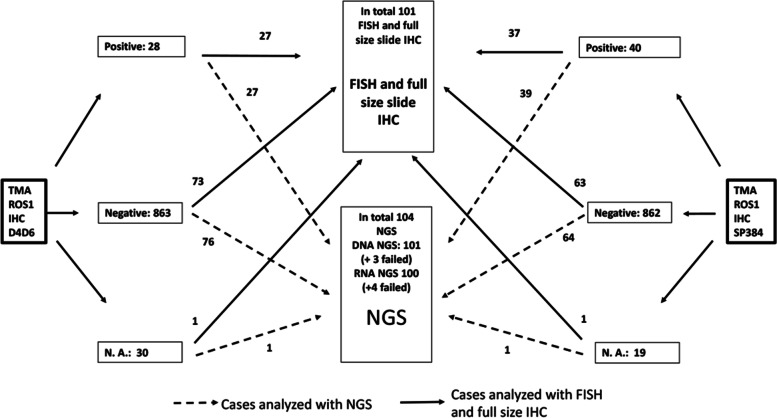
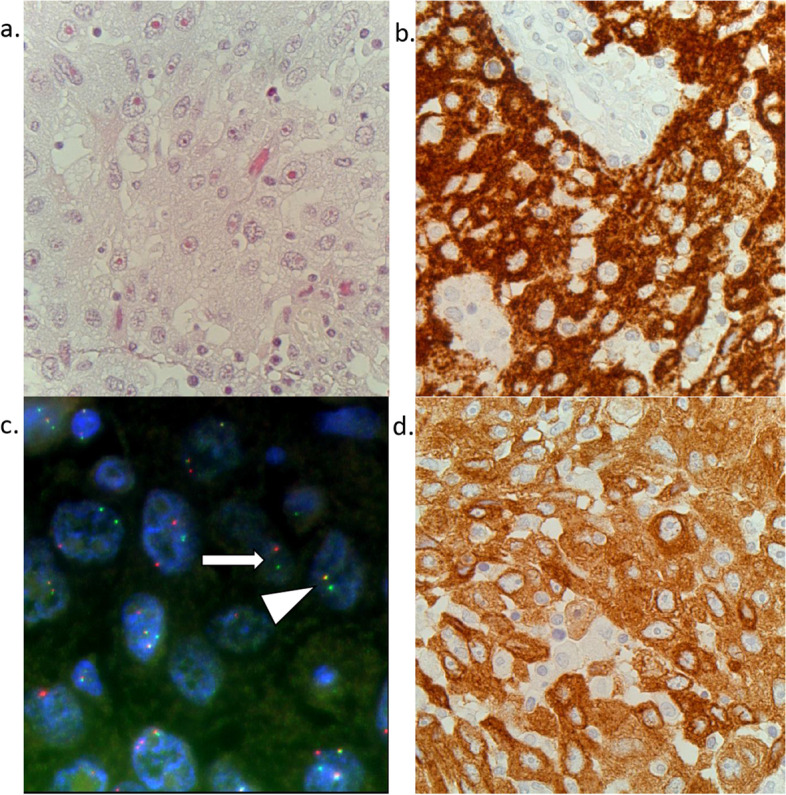
The study was performed using biobank material from 921 lung cancer patients including 542 patients with adenocarcinoma surgically resected during 2006-2018. Initially, we screened the samples with two different IHC clones (D4D6 and SP384) targeting ROS1. All samples that showed more than weak or focal staining, as well as a subgroup of negative samples, were analyzed with ROS1 fluorescence in situ hybridization (FISH) and next-generation sequencing (NGS) with a comprehensive NGS DNA and RNA panel. Positive ROS1-fusion was defined as those samples positive in at least two of the three methods (IHC, FISH, NGS).
Fifty cases were IHC positive. Of these, three samples were both NGS and FISH-positive and considered positive for ROS1 fusion. Two more samples were FISH positive only, and whilst IHC and NGS were negative. These were also negative with Reverse Transcription quantitative real time Polymerase Chain Reaction (RT-qPCR). The prevalence of ROS1 fusion in adenocarcinomas was 0.6%. All cases with ROS1 fusion had TP53 mutations. IHC-positivity was associated with adenocarcinoma. Among SP384-IHC positive cases we also found an association with never smoking status. There was no association between positive IHC and overall survival, time to relapse, age, stage, sex or pack-year of smoking.
ROS1 seems to be less frequent in early-stage disease than in advanced stages. IHC is a sensitive, but less specific method and the results need to be confirmed with another method like FISH or NGS.
ROS1 融合是转移性非小细胞肺癌患者治疗的一个罕见但有吸引力的靶点。在主要针对晚期疾病的研究中,ROS1 融合的患病率约为 1-3%。在早期肺癌中,ROS1 也可能为新辅助或辅助治疗提供一个富有成效的靶点。在本研究中,我们调查了挪威早期肺癌患者队列中 ROS1 融合的患病率。我们还探讨了 ROS1 免疫组织化学(IHC)染色阳性是否与某些突变、临床特征和结局相关。
该研究使用了来自 921 名肺癌患者的生物库材料,其中包括 542 名在 2006 年至 2018 年期间接受手术切除的腺癌患者。最初,我们使用针对 ROS1 的两种不同的 IHC 克隆(D4D6 和 SP384)对样本进行筛选。所有显示强或局灶性染色的样本,以及亚组阴性样本,均进行 ROS1 荧光原位杂交(FISH)和下一代测序(NGS)分析,采用全面的 NGS DNA 和 RNA 面板。ROS1 融合阳性定义为至少两种三种方法(IHC、FISH 和 NGS)均阳性的样本。
50 例 IHC 阳性。其中,3 例样本 NGS 和 FISH 均阳性,被认为 ROS1 融合阳性。另外 2 例仅 FISH 阳性,而 IHC 和 NGS 均为阴性。这些样本的逆转录实时定量聚合酶链反应(RT-qPCR)也是阴性的。腺癌中 ROS1 融合的患病率为 0.6%。所有 ROS1 融合病例均存在 TP53 突变。IHC 阳性与腺癌有关。在 SP384- IHC 阳性病例中,我们还发现与从不吸烟状态有关。IHC 阳性与总生存时间、复发时间、年龄、分期、性别或吸烟包年数之间无相关性。
ROS1 在早期疾病中的频率似乎低于晚期。IHC 是一种敏感但特异性较低的方法,结果需要通过 FISH 或 NGS 等另一种方法来确认。